Anti-Inflammatory Injections Can't Cure Rosacea? The Vicious Cycle of Inflammation and Angiogenesis
The logic seems straightforward: rosacea is an inflammatory disease, so anti-inflammatory treatment should fix it. Your doctor administers a corticosteroid injection or a potent anti-inflammatory cocktail into the affected area. Within days, the redness fades, the burning subsides, and you feel like the condition has finally been addressed at its root. Three weeks later, the redness is back — often with a vengeance.
This pattern of dramatic temporary improvement followed by aggressive rebound is not a coincidence. It reveals something fundamental about rosacea that many treatment approaches fail to account for: inflammation and blood vessel formation in rosacea are not independent problems. They are locked in a self-reinforcing cycle where each drives the other, and suppressing one without addressing the connection between them guarantees recurrence.
Table of Contents
- The Inflammation-Angiogenesis Feedback Loop Explained
- Why Corticosteroid Injections Fail for Rosacea Long-Term
- The Rebound Phenomenon: Worse Than Before Treatment
- Breaking the Cycle vs. Suppressing Symptoms: A Critical Distinction
- What Happens at the Molecular Level During a Rosacea Flare
- Toward Disease Modification: Approaches That Target the Cycle Itself
The Inflammation-Angiogenesis Feedback Loop Explained {#feedback-loop-explained}
To understand why anti-inflammatory injections cannot cure rosacea, you first need to understand the relationship between inflammation and angiogenesis (new blood vessel formation) in this disease.
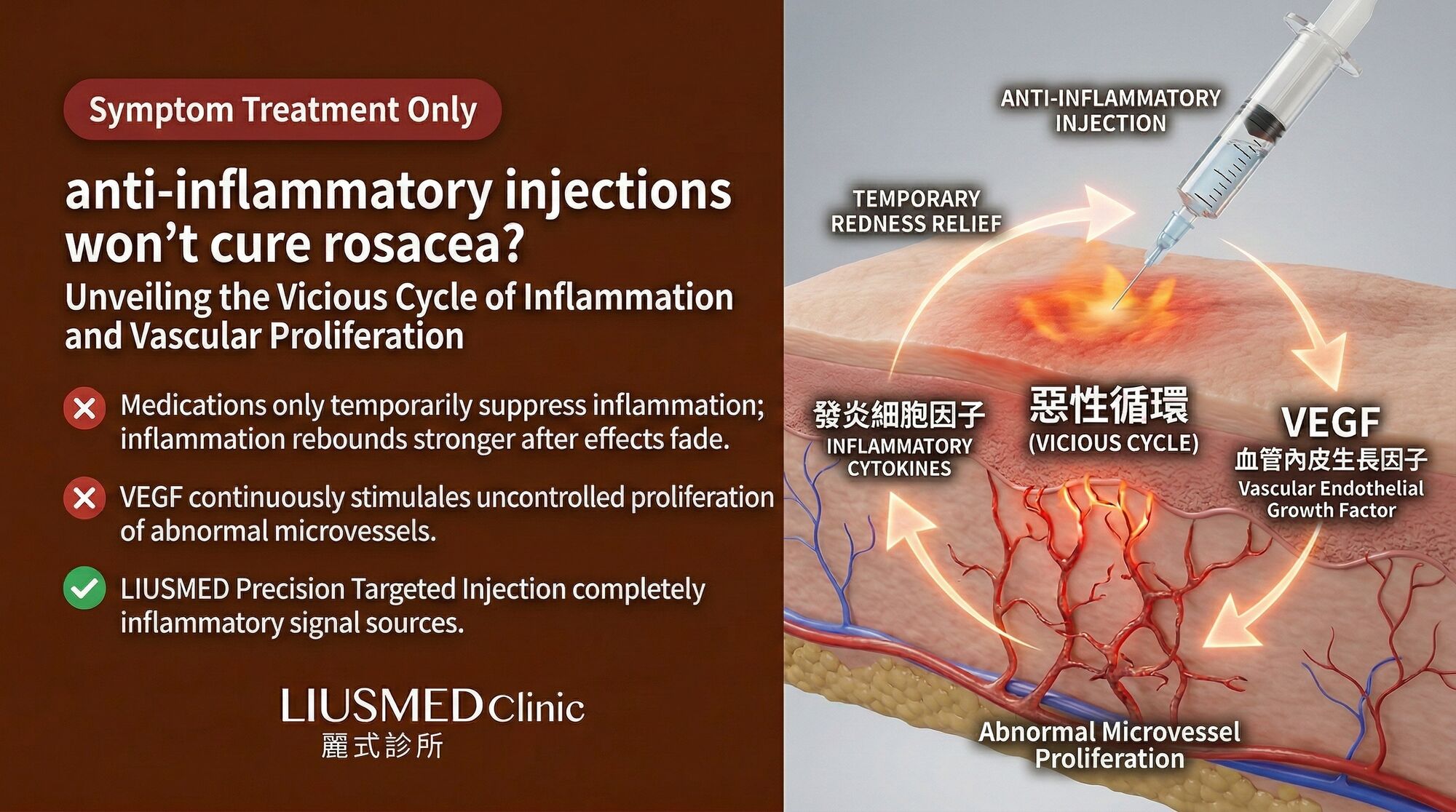
In healthy tissue, inflammation and angiogenesis are linked but tightly controlled processes. When tissue is injured, inflammation recruits immune cells that clean up damage and release growth factors — including VEGF (Vascular Endothelial Growth Factor — new blood vessel signal) — that stimulate new blood vessel growth to supply the healing tissue. Once healing is complete, both inflammation and angiogenesis resolve, and the tissue returns to homeostasis.
In rosacea, this resolution never fully occurs. The cycle becomes self-sustaining:
Step 1: Chronic inflammation produces pro-angiogenic signals. Inflammatory cells in rosacea skin — mast cells, macrophages, T-cells — continuously produce VEGF, fibroblast growth factor (FGF), and other angiogenic mediators. This is not wound-healing angiogenesis; it is pathological angiogenesis driven by a chronically activated immune system.
Step 2: New blood vessels amplify inflammation. Each new vessel is not just a passive conduit for blood flow. Endothelial cells in newly formed vessels are immunologically active — they express adhesion molecules that recruit more inflammatory cells from the bloodstream, produce their own cytokines, and create a permeable vascular surface through which inflammatory mediators leak into surrounding tissue.
Step 3: Amplified inflammation drives more angiogenesis. The additional inflammatory cells recruited through the new vessels produce more VEGF and other angiogenic signals, stimulating yet more vessel formation. The cycle accelerates.
Step 4: Structural changes prevent resolution. As the vessel network expands, it creates a physical infrastructure that sustains inflammation even during periods of reduced triggering. The vessels are permanent until destroyed; the inflammatory cells they recruit are continuously renewed.
This is the vicious cycle. Inflammation drives vessel formation; vessels amplify inflammation; amplified inflammation drives more vessels. An intervention that temporarily suppresses inflammation without disrupting this feedback loop provides temporary relief while the structural component (the expanded vascular network) remains intact, ready to restart the cycle the moment suppression is lifted.
Why Corticosteroid Injections Fail for Rosacea Long-Term {#corticosteroid-injections-fail}
Corticosteroids are powerful anti-inflammatory agents. Injected into rosacea-affected skin, they suppress multiple inflammatory pathways simultaneously — inhibiting prostaglandin synthesis, reducing cytokine production, stabilizing mast cell membranes, and decreasing immune cell recruitment. The effect is rapid and dramatic.
However, corticosteroids have no direct anti-angiogenic effect. In fact, the relationship between corticosteroids and angiogenesis is complex and, in some contexts, paradoxical:
During active treatment: Corticosteroids reduce VEGF production indirectly by suppressing the inflammatory cells that produce it. This reduces the angiogenic drive, but only for as long as the anti-inflammatory effect persists. Existing vessels are not affected — they remain patent and functional.
After treatment wears off: When corticosteroid levels drop (typically 2–4 weeks after injection), the inflammatory cells that were suppressed reactivate. But they reactivate in an environment where the expanded vascular network is still intact. The vessels immediately begin recruiting inflammatory cells at the amplified rate determined by the size of the vascular network — which has not changed.
Rebound angiogenesis: There is evidence that withdrawal from corticosteroid suppression triggers a compensatory surge in angiogenic signaling, as the tissue responds to the relative absence of the suppressive signal. This "angiogenic rebound" can result in more vessel formation in the weeks following corticosteroid wear-off than was present before treatment.
Structural dermal damage: Repeated corticosteroid injections cause well-documented tissue atrophy — thinning of the dermis, loss of subcutaneous fat, and weakening of connective tissue. In rosacea skin that may already have a compromised dermal matrix, this adds structural damage to the existing inflammatory and vascular pathology.
The net trajectory of repeated corticosteroid injections for rosacea is therefore: temporary improvement followed by return to baseline or worse, with progressive structural deterioration of the treated tissue. This is not treatment failure in the sense that the drug did not work — the anti-inflammatory effect was genuine. It is a failure of the treatment strategy to address the self-reinforcing nature of the disease.
The Rebound Phenomenon: Worse Than Before Treatment {#rebound-phenomenon}
The rebound following anti-inflammatory injection withdrawal deserves detailed examination, as it is one of the most distressing experiences rosacea patients report.
Rebound occurs because suppression and resolution are fundamentally different biological processes:
Suppression holds inflammatory activity at artificially low levels while the underlying drivers remain active. When the suppressive agent is removed, all drivers resume simultaneously.
Resolution is an active biological process involving specialized pro-resolving mediators (resolvins, lipoxins, protectins) that reprogram inflammatory cells, clear inflammatory debris, and restore homeostatic signaling. Resolution actually changes the tissue state.
Corticosteroid injections achieve suppression, not resolution. When the drug wears off, multiple inflammatory pathways reactivate simultaneously — like releasing a compressed spring. The tissue experiences a rapid, coordinated inflammatory surge that often exceeds the pre-treatment state because:
- Suppressed mast cells that accumulated inflammatory mediators during treatment release them en masse during rebound
- The vascular network (unchanged by treatment) rapidly fills with newly recruited inflammatory cells
- Neurogenic inflammatory pathways, suppressed during treatment, reactivate with heightened sensitivity
- The corticosteroid-induced structural damage (dermal thinning) reduces the tissue's mechanical resistance to vasodilation
Patients frequently describe the rebound as their "worst flare ever" — and from both a clinical and molecular perspective, this assessment is often accurate. The combination of inflammatory rebound through an intact expanded vascular network, in structurally compromised tissue, produces a flare of unusual intensity and duration.
| Phase | Redness | Burning/Stinging | Papules/Pustules | Duration |
|---|---|---|---|---|
| Pre-treatment baseline | Moderate-severe | Intermittent | Variable | Chronic |
| During corticosteroid effect | Minimal-mild | Absent or mild | Usually cleared | 2–4 weeks |
| Early rebound (week 1) | Severe, often exceeds baseline | Intense, often constant | May erupt even if not previously present | Days to weeks |
| Late rebound (weeks 2–4) | Gradually returning toward new baseline | Moderating but often worse than pre-treatment | Variable | Weeks |
| New baseline | Equal to or worse than pre-treatment | Often worse than pre-treatment | May have shifted disease subtype | Chronic |
Breaking the Cycle vs. Suppressing Symptoms: A Critical Distinction {#breaking-vs-suppressing}
The failure of anti-inflammatory injections highlights a critical distinction in rosacea treatment philosophy: the difference between suppressing symptoms and breaking the disease cycle.
Symptom suppression addresses the downstream effects of the disease — redness, burning, papules — without modifying the upstream mechanisms that produce them. Corticosteroids, antihistamines, vasoconstrictors, and short-course antibiotics are symptom suppressors. They provide relief during their period of activity but do not change the disease trajectory.
Cycle breaking targets the connections between inflammation and angiogenesis — the feedback mechanisms that make the disease self-sustaining. This requires simultaneously addressing:
- The inflammatory drive (reducing cytokine production, modulating immune cell behavior)
- The angiogenic response (reducing VEGF signaling, stabilizing existing vessels)
- The vascular amplification of inflammation (improving vessel maturity, reducing permeability)
- The structural support (repairing the dermal matrix to provide mechanical resistance to vasodilation)
No single agent addresses all four of these nodes. This is why monotherapy for rosacea — whether it is a steroid, an antibiotic, or a laser — consistently underperforms patient expectations. The disease is a system, and treating one component while leaving the others intact allows the system to regenerate.
Effective rosacea management requires a coordinated multi-target approach that weakens the cycle at multiple points simultaneously. When the inflammatory drive is reduced at the same time that angiogenic signaling is dampened and vascular stability is improved, the self-reinforcing loop can be weakened enough for the tissue to begin moving toward resolution rather than perpetual cycling.
What Happens at the Molecular Level During a Rosacea Flare {#molecular-level-flare}
Understanding the molecular cascade during a flare illustrates why the inflammation-angiogenesis cycle is so difficult to break:
Trigger exposure (heat, stress, alcohol, UV, exercise) activates TRP channels (TRPV1, TRPA1) on sensory nerve endings in rosacea-affected skin. These channels have a lower activation threshold in rosacea due to chronic sensitization.
Neuropeptide release follows within seconds. Substance P and CGRP (Calcitonin Gene-Related Peptide) are released from nerve endings, causing immediate arteriolar vasodilation and increasing capillary permeability. This is the initial flush.
Mast cell degranulation occurs within minutes. Neuropeptides trigger mast cells to release histamine, tryptase, TNF-alpha, and VEGF. Histamine causes further vasodilation; tryptase activates protease-activated receptors (PARs) on endothelial cells; TNF-alpha recruits neutrophils; VEGF signals endothelial cells to proliferate.
Neutrophil infiltration begins within hours. Neutrophils migrate through the permeable vessel walls, releasing reactive oxygen species and MMP (Matrix Metalloproteinase)-9 that damage the extracellular matrix and release additional matrix-bound VEGF.
Cathelicidin activation amplifies within 12–24 hours. Kallikrein-5 processes cathelicidin into LL-37, a potent pro-inflammatory and pro-angiogenic peptide. LL-37 activates formyl peptide receptors on immune cells, further amplifying the inflammatory response.
Endothelial activation becomes prominent by 24–48 hours. Endothelial cells in dilated vessels upregulate adhesion molecules (ICAM-1, VCAM-1, E-selectin), increasing their capacity to recruit inflammatory cells from the bloodstream.
Angiogenic sprouting begins within days. The sustained VEGF signal from multiple sources (mast cells, macrophages, neutrophil-released matrix-bound VEGF, LL-37-stimulated keratinocytes) initiates endothelial cell proliferation and vessel sprouting. New vessel tips extend toward the VEGF gradient.
Vessel maturation failure is characteristic of rosacea. The new vessels form without adequate pericyte recruitment (partly due to the inflammatory environment, partly due to elevated MMP-9 degrading PDGF-BB), resulting in immature, leaky, unstable vessels that amplify the next cycle.
The entire cascade — from trigger to new unstable vessels — occurs within one to two weeks. The new vessels then become permanent participants in future cycles, progressively expanding the vascular network and amplifying each subsequent flare.
Toward Disease Modification: Approaches That Target the Cycle Itself {#disease-modification-approaches}
True disease modification in rosacea requires interventions that interrupt the feedback loop rather than temporarily suppressing its output. Several principles guide effective cycle-breaking strategies:
Simultaneous multi-target intervention. Addressing inflammation alone (as with corticosteroids) or vessels alone (as with laser) leaves the cycle intact. Effective approaches combine anti-inflammatory action with anti-angiogenic action and structural support. This is the rationale behind comprehensive protocols like Rosacea Injection Treatment, which delivers multiple active agents to the affected tissue simultaneously.
Sustained rather than pulsed treatment. The inflammation-angiogenesis cycle operates continuously. Pulsed interventions (a single injection, a single laser session) create temporary disruptions followed by full cycle recovery. Sustained intervention — maintaining therapeutic levels of cycle-disrupting agents over weeks to months — gives the tissue time to structurally remodel away from the pathological state.
Promoting resolution rather than suppression. Emerging approaches focus on supporting the body's natural pro-resolving mechanisms — enhancing production of specialized pro-resolving mediators, supporting regulatory T-cell function, and promoting macrophage phenotype switching from M1 (pro-inflammatory) to M2 (pro-resolving). These approaches promote genuine tissue healing rather than artificial symptom suppression.
Vessel stabilization rather than destruction. Rather than destroying vessels and allowing the angiogenic drive to replace them with worse ones, stabilization approaches aim to mature existing vessels — improving pericyte coverage, strengthening basement membranes, and reducing endothelial permeability. Stable, mature vessels recruit fewer inflammatory cells and produce fewer pro-angiogenic signals than immature, leaky ones.
Progressive de-escalation. Once the cycle begins to weaken — evidenced by reduced flare frequency, lower baseline redness, and improved trigger tolerance — treatment intensity can be gradually reduced. This is fundamentally different from the corticosteroid pattern where cessation triggers immediate rebound. A weakened cycle recovers more slowly, allowing progressive treatment reduction without loss of gains.
The goal is not to suppress rosacea into temporary silence but to weaken the feedback loop sufficiently that the tissue can sustain a new, lower-inflammation equilibrium. This is a longer process than a single injection, but it produces durable improvement that does not depend on continuous pharmacological suppression.
Frequently Asked Questions
Q1: My doctor gave me a steroid injection for a severe rosacea flare. Was that wrong?
Not necessarily. In the context of a severe acute flare causing significant distress, a single corticosteroid injection can provide meaningful symptomatic relief and is a reasonable crisis intervention. The problem is not the single rescue injection but the pattern of relying on repeated injections as a management strategy. A single injection to break a severe flare, followed by implementation of a cycle-targeting maintenance plan, is different from quarterly steroid injections as ongoing rosacea management.
Q2: Are all anti-inflammatory injections problematic for rosacea, or just steroids?
Corticosteroids carry the specific risks of tissue atrophy and steroid-induced rosacea with repeated use. Non-steroidal anti-inflammatory injections may avoid these specific complications but still face the fundamental limitation of suppressing inflammation without breaking the angiogenesis feedback loop. Any anti-inflammatory agent that does not simultaneously address the vascular component of the cycle will provide temporary benefit followed by recurrence.
Q3: How long does the rebound effect last after stopping steroid injections?
Rebound duration depends on the potency and dose of the corticosteroid used, the duration of treatment, and the severity of underlying rosacea. After a single injection of a moderate-potency corticosteroid, rebound typically peaks at one to two weeks post-wear-off and settles over four to six weeks. After repeated or high-potency steroid exposure, rebound can persist for two to three months, and some patients develop steroid-induced rosacea that requires its own separate treatment course.
Q4: Can oral anti-inflammatory medications break the cycle better than injections?
Oral anti-inflammatory medications (such as low-dose doxycycline at anti-inflammatory doses) address systemic inflammation and can modulate the inflammatory component of the cycle. However, they also do not directly address the vascular component. Their advantage over injections is sustained rather than pulsed delivery, which avoids the dramatic rebound cycle. Their limitation is that systemic delivery means only a fraction of the active agent reaches the affected facial tissue. The combination of targeted local delivery with systemic support often outperforms either alone.
Q5: If the cycle is self-reinforcing, how does rosacea ever go into remission naturally?
Natural remission, which does occur in some patients, typically results from changes in the balance of the cycle rather than a specific intervention. Hormonal shifts, lifestyle modifications, stress reduction, climate changes, and immune system maturation with age can all shift the inflammatory-angiogenic balance enough for the cycle to slow. The vessels remain, but if the inflammatory drive decreases enough, the amplification effect weakens and a new, lower-activity equilibrium can establish. This is why some patients experience improvement in their 40s or 50s after decades of active disease.
Q6: What should I ask my doctor about before accepting anti-inflammatory injections for rosacea?
Key questions include: What specific agent will be injected, and what are its effects on angiogenesis? Is this intended as a one-time rescue or an ongoing management strategy? What is the plan for addressing the vascular component of my rosacea? How will we prevent rebound after the injection wears off? What cycle-breaking strategies can we implement alongside or instead of repeated injections? A practitioner who can answer these questions thoughtfully is approaching rosacea as a systemic disease rather than a simple inflammation to be suppressed.
About the Author
Dr. Ta-Ju Liu is the founder of Liusmed Clinic, a specialized practice focused on regenerative medicine and minimal incision surgery. Dr. Liu's approach to rosacea is grounded in understanding the disease as a self-reinforcing inflammatory-vascular cycle that requires multi-target intervention. Liusmed Clinic develops treatment protocols that aim for genuine disease modification rather than symptom suppression, serving patients from Taiwan and internationally who seek lasting improvement in chronic rosacea.
Disclaimer
This article is provided for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Corticosteroid injections and other anti-inflammatory treatments are established medical therapies with legitimate clinical applications. This article discusses their limitations specifically in the context of chronic rosacea management. Individual responses to treatment vary. All treatment decisions should be made in consultation with a qualified healthcare provider.

Specialties
Credentials
- Kaohsiung Medical University, School of Medicine
- Attending Physician, Dermatology, Kaohsiung Chang Gung Memorial Hospital
- Attending Physician, Aesthetic Center, Kaohsiung Chang Gung Memorial Hospital
- Visiting Physician, Dermatology, Xiamen Chang Gung Hospital
- Visiting Physician, Aesthetic Center, Xiamen Chang Gung Hospital
"For every surgery, I strive to achieve a good outcome through a small incision and refined technique. Minimally invasive surgery is not just a technique — it's a commitment of respect to every patient."
Recovery after any procedure needs peer support too
Want to learn more?
Schedule a consultation for professional evaluation and advice