Liusmed Non-Laser Rosacea Injection vs Traditional Laser
If you have been living with rosacea for years, you have probably heard the same advice on repeat: pulsed dye laser, IPL (Intense Pulsed Light), vascular laser, more laser. The standard dermatology playbook treats rosacea as a problem of visible blood vessels and prescribes photon-based destruction as the primary solution. Yet many patients return session after session, watching their redness fade temporarily only to creep back within weeks. The reason is deceptively simple -- destroying vessels without repairing the tissue that allowed them to proliferate in the first place is treating the symptom while ignoring the disease.
At Liusmed Clinic, we asked a different question: what if instead of burning away the consequences of barrier dysfunction, we rebuilt the barrier itself?
Table of Contents
- The Conventional Laser Paradigm and Its Limitations
- Understanding Rosacea as a Barrier Disease
- The Liusmed Non-Laser Skin Remodeling Injection Protocol
- Laser Therapy vs. Injection Remodeling: A Head-to-Head Comparison
- Clinical Outcomes and What to Expect
- Who Is a Good Candidate for the Injection Protocol
The Conventional Laser Paradigm and Its Limitations
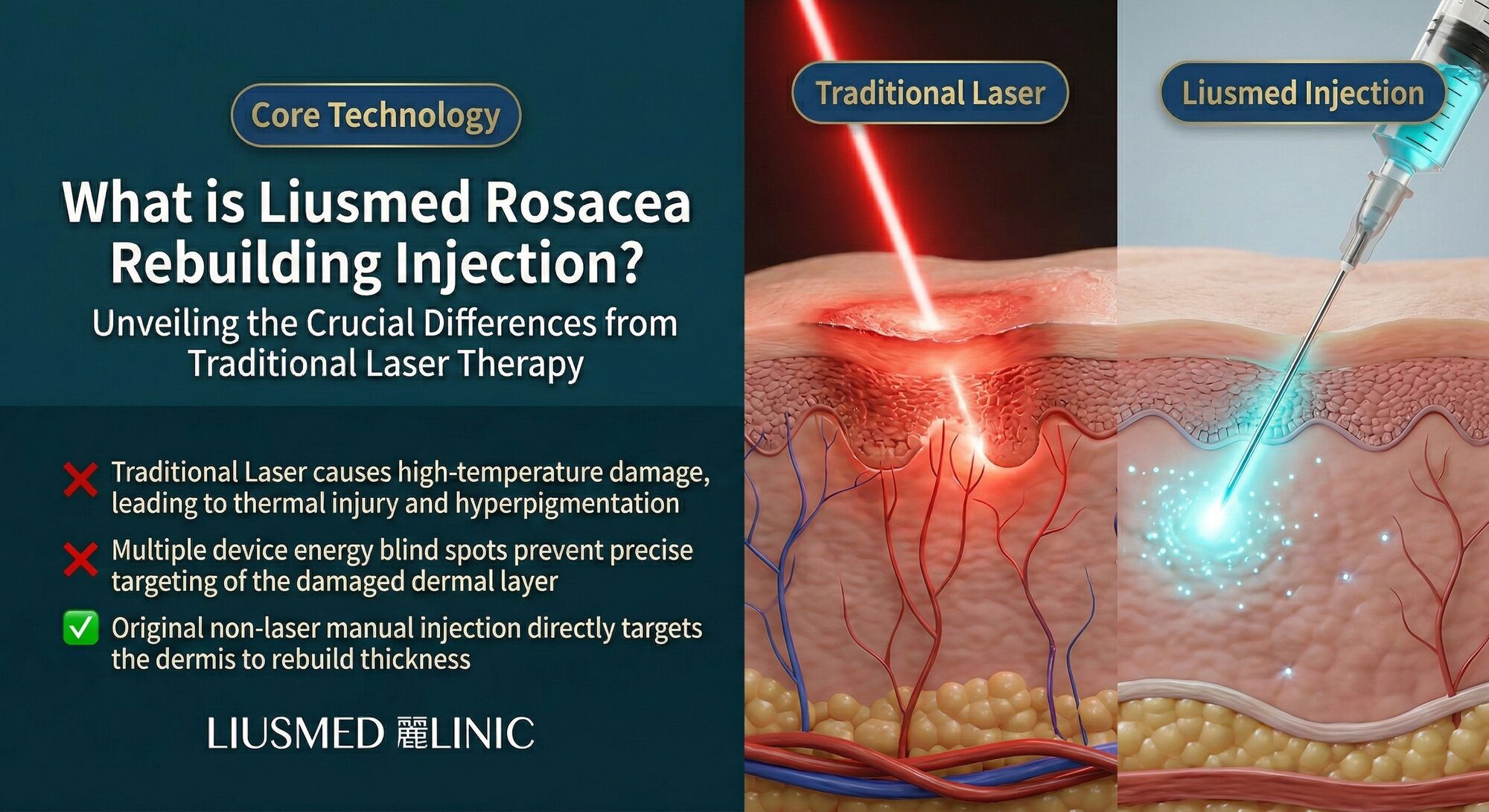
Laser and intense pulsed light (IPL) therapies have dominated rosacea management for over two decades. The principle is straightforward: selective photothermolysis targets oxyhemoglobin inside dilated blood vessels, heats them until they coagulate, and the body reabsorbs the damaged vessel over the following weeks. For patients with prominent telangiectasia, the cosmetic improvement can be dramatic in the short term.
However, the laser paradigm has several structural weaknesses that are rarely discussed during consultation:
- Thermal collateral damage. Even well-calibrated devices deposit heat into surrounding tissue. In rosacea skin, where the epidermal barrier is already compromised, additional thermal insult can trigger post-inflammatory erythema and paradoxical flushing.
- Neovascularization rebound. When vessels are destroyed without addressing the underlying VEGF (vascular endothelial growth factor) signaling, the body often rebuilds them. Patients frequently require maintenance sessions every three to six months indefinitely.
- No barrier repair. Laser energy does nothing to restore the thinned dermis, disrupted basement membrane, or depleted extracellular matrix that characterize rosacea-affected skin. The structural deficit remains.
- Neurogenic inflammation. Rosacea involves overactive sensory neurons releasing substance P and CGRP (Calcitonin Gene-Related Peptide). Laser heat can actually stimulate these nerve endings, worsening the neuroinflammatory cycle in sensitive patients.
These limitations do not mean lasers have no role. They mean that a laser-only strategy addresses downstream consequences while leaving the upstream pathology untouched.
Understanding Rosacea as a Barrier Disease
Contemporary research increasingly frames rosacea not simply as a vascular disorder but as a disease of barrier dysfunction and innate immune dysregulation. Several key tissue-level changes define the rosacea phenotype:
Basement membrane disruption. The dermo-epidermal junction in rosacea patients shows fragmentation of collagen IV and laminin networks. This allows inflammatory mediators to pass more freely between the dermis and epidermis and permits abnormal vessel sprouting.
Dermal thinning. Chronic inflammation degrades collagen I and III in the papillary dermis. The resulting thin dermis makes underlying vessels more visible -- what we perceive as persistent redness is partly a translucency problem, not just a vessel problem.
Cathelicidin and kallikrein overexpression. The innate immune peptide LL-37 is overproduced in rosacea skin, driving both inflammation and angiogenesis. Kallikrein 5, a serine protease, cleaves cathelicidin into its active inflammatory form.
Mast cell activation. Mast cells in the perivascular space degranulate more readily in rosacea, releasing histamine, tryptase, and VEGF (Vascular Endothelial Growth Factor — new blood vessel signal). This creates a self-reinforcing loop of vessel dilation, leakage, and new vessel formation.
Understanding these mechanisms makes it clear why surface-level vessel destruction provides only temporary relief. The tissue environment that generates abnormal vasculature remains fully intact after every laser session.
The Liusmed Non-Laser Skin Remodeling Injection Protocol
The Rosacea Injection Treatment developed at Liusmed Clinic is built on a fundamentally different therapeutic logic: rather than destroying pathological vessels from the outside, we deliver a precise cocktail of agents directly into the affected dermal layers to suppress the signals that create those vessels and simultaneously rebuild the structural matrix that has been lost.
The protocol involves manual mesotherapy injection -- not machine-driven meso guns -- to deliver a customized formulation that typically includes:
- Tranexamic acid (TXA): An anti-plasmin agent that blocks plasminogen activation, reducing VEGF release and suppressing the angiogenic cascade at its source.
- Dilute botulinum toxin (microbotox): At sub-muscular doses, botulinum toxin inhibits acetylcholine release from autonomic nerve terminals in the dermis, reducing neurogenic vasodilation and sebaceous gland overactivity.
- PRP (Platelet-Rich Plasma) or PLT (Platelet (count)) growth factors: Concentrated platelet-derived growth factors stimulate fibroblast proliferation, collagen synthesis, and basement membrane component production -- directly rebuilding what rosacea has degraded.
Each component addresses a different node in the rosacea pathology network. The combined effect is anti-angiogenic, anti-inflammatory, and pro-regenerative -- a three-pronged approach that no single laser wavelength can replicate.
Laser Therapy vs. Injection Remodeling: A Head-to-Head Comparison
| Parameter | Traditional Laser / IPL | Liusmed Injection Protocol |
|---|---|---|
| Primary mechanism | Photothermal vessel destruction | Multi-target biochemical remodeling |
| Basement membrane repair | None | Active restoration via growth factors |
| VEGF suppression | Indirect (vessel removal) | Direct (TXA blocks angiogenic signaling) |
| Neurogenic inflammation | May worsen (thermal stimulation) | Reduced (microbotox calms neural firing) |
| Dermal collagen rebuilding | Minimal (some remodeling from heat) | Significant (PRP/PLT fibroblast activation) |
| Downtime | 3-7 days redness and swelling | Mild pinpoint redness for 24-48 hours |
| Session frequency | Every 3-6 months ongoing | Tapering schedule toward independence |
| Suitable for thin / sensitive skin | Higher risk of burns and PIH | Lower risk; no thermal energy involved |
| Pain level | Moderate to significant (snapping sensation) | Mild (topical numbing used) |
| Long-term vessel recurrence | Common without maintenance | Reduced as barrier function improves |
The comparison highlights a philosophical divide: laser therapy is primarily destructive, while the injection protocol is primarily constructive. Both reduce visible redness, but through opposing mechanisms.
Clinical Outcomes and What to Expect
Patients undergoing the Liusmed injection protocol typically follow a structured treatment timeline:
Weeks 1-4 (Loading phase): Sessions are spaced one to two weeks apart. During this phase, the primary goals are inflammation suppression and initial VEGF reduction. Many patients notice reduced flushing frequency and decreased skin sensitivity within the first two sessions.
Months 2-3 (Remodeling phase): Session spacing extends to every three to four weeks. The focus shifts toward dermal rebuilding as growth factors stimulate new collagen deposition. Skin texture and thickness improve, and the translucency that amplifies visible redness begins to diminish.
Months 4-6 (Tapering phase): Treatment intervals lengthen progressively. The goal is gradual independence from the protocol as the remodeled tissue maintains its own structural integrity. Not all patients reach full independence, but most achieve a significantly reduced maintenance frequency compared to laser-dependent schedules.
Clinical photography under standardized lighting conditions is used to track changes in erythema distribution, vessel density, and overall skin quality at each visit. Patients are encouraged to maintain a flushing diary to document trigger responses, which typically decrease as barrier function improves.
Who Is a Good Candidate for the Injection Protocol
The injection protocol is particularly well-suited for:
- Patients with erythematotelangiectatic rosacea (ETR) who have not responded satisfactorily to laser therapy or who experience post-laser rebound flushing.
- Patients with papulopustular rosacea in whom the inflammatory component dominates over fixed telangiectasia.
- Patients with thin or sensitive skin for whom laser energy poses an unacceptable risk of thermal injury or post-inflammatory hyperpigmentation.
- Patients seeking a long-term structural solution rather than indefinite cosmetic maintenance.
- Patients who have been through multiple courses of topical therapy (metronidazole, azelaic acid, ivermectin) without achieving lasting improvement.
Patients with very prominent, large-caliber telangiectasia may still benefit from targeted laser treatment for those specific vessels, followed by the injection protocol to address underlying barrier dysfunction and prevent recurrence. The two modalities are not mutually exclusive -- but the injection protocol addresses the disease layer that lasers cannot reach.
If you are exploring alternatives to the conventional laser cycle, the Rosacea Injection Treatment at Liusmed Clinic may offer the tissue-level repair your skin has been missing.
Frequently Asked Questions
Q1: Is the Liusmed injection protocol a replacement for all laser treatments?
Not necessarily. For patients with isolated large-caliber telangiectasia, a single targeted laser session may still be appropriate to remove those specific vessels. However, the injection protocol addresses the underlying barrier dysfunction and angiogenic signaling that lasers do not. Many patients find that after completing the injection protocol, their need for laser maintenance is dramatically reduced or eliminated entirely.
Q2: How painful is the injection compared to laser therapy?
Most patients report that the injection protocol is less painful than laser treatment. A topical anesthetic cream is applied before each session, and the manual injection technique uses very fine needles. Patients typically describe a mild pricking sensation rather than the sharp snapping or burning feeling associated with laser pulses.
Q3: Can I receive the injection protocol if I am currently using topical rosacea medications?
Yes. Most topical rosacea medications (metronidazole, azelaic acid, ivermectin) can be continued during the injection protocol. In some cases, your physician may adjust the topical regimen as your skin improves. Patients on oral isotretinoin should discuss timing with their provider, as this medication affects wound healing.
Q4: How many sessions are typically needed before visible improvement?
Many patients notice a reduction in flushing frequency and skin sensitivity within two to three sessions. Visible reduction in background redness typically becomes apparent by the fourth to sixth session. Full structural remodeling and maximal improvement usually require twelve to sixteen sessions over four to six months.
Q5: Will my rosacea come back after I finish the protocol?
Rosacea is a chronic condition with a genetic component, so complete permanent elimination is not a realistic promise from any treatment. However, patients who complete the full tapering protocol often maintain their improvement for significantly longer periods than those relying on laser alone, because the structural barrier has been rebuilt rather than merely cosmetically managed. Annual maintenance sessions may be recommended.
Q6: Is this protocol suitable for rosacea affecting the nose (phymatous rosacea)?
Phymatous changes such as rhinophyma involve significant tissue hypertrophy and fibrosis that may require surgical intervention. The injection protocol is most effective for erythematotelangiectatic and papulopustular subtypes. However, it can be used as an adjunctive treatment to reduce inflammation and improve skin quality in early phymatous rosacea before surgical thresholds are reached.
About the Author
Dr. Ta-Ju Liu is the founder of Liusmed Clinic, a specialized practice focused on regenerative medicine and minimal incision surgery. With extensive clinical experience in dermal remodeling, growth factor therapy, and mesotherapy injection techniques, Dr. Liu developed the Liusmed rosacea injection protocol to address the structural tissue deficits that conventional laser therapy leaves untreated. His approach integrates evidence-based pharmacology with precision manual injection to deliver targeted, tissue-level repair for chronic skin conditions.
Disclaimer
This article is provided for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Individual results may vary. Rosacea is a complex medical condition that requires professional evaluation. Always consult a qualified healthcare provider before beginning any new treatment. The information presented reflects the clinical perspective and protocols used at Liusmed Clinic and may not be applicable to all patients or clinical settings.

Specialties
Credentials
- Kaohsiung Medical University, School of Medicine
- Attending Physician, Dermatology, Kaohsiung Chang Gung Memorial Hospital
- Attending Physician, Aesthetic Center, Kaohsiung Chang Gung Memorial Hospital
- Visiting Physician, Dermatology, Xiamen Chang Gung Hospital
- Visiting Physician, Aesthetic Center, Xiamen Chang Gung Hospital
"For every surgery, I strive to achieve a good outcome through a small incision and refined technique. Minimally invasive surgery is not just a technique — it's a commitment of respect to every patient."
Recovery after any procedure needs peer support too
Want to learn more?
Schedule a consultation for professional evaluation and advice