Male Intimate Shockwave + PRP — A Complete Guide: EAU Guidelines, LI-SWT Systematic Reviews, and Treatment-Room Privacy Protocol
Summary
Male erectile dysfunction (ED — difficulty maintaining erection**)** has a prevalence of roughly 16–17% in men over 40, yet only about 10% seek medical help. Shame, fear of pain, and uncertainty about efficacy are the three main barriers to care. This article uses the European EAU (European Association of Urology) guideline, LI-SWT (Low-Intensity Shockwave Therapy — sound-wave pulses inducing new blood vessels) systematic reviews, and Liusmed Clinic's treatment-room-clear protocol as its anchors to explain the evidence boundaries, process design, and risk disclosure of shockwave + PRP (Platelet-Rich Plasma — concentrate of your own blood platelets rich in growth factors) — helping you make an informed decision.
Low-intensity shockwave was formally approved by Taiwan MOHW for ED in 2015; the Taiwan Andrological Association listed it the same year as a first-line treatment option or adjunct to oral medication, and EAU incorporated it into guidelines in 2015. Taiwan clinical satisfaction averages ~75%; local cohort research (Tzou 2021, PMID — PubMed Identifier, unique paper ID in PubMed database — 34829899) shows significant IIEF (International Index of Erectile Function)-5 (International Index of Erectile Function — 5-item erectile function questionnaire), EHS and quality-of-life improvement after 12 sessions (p<0.001). Evidence for PRP in ED is steadily accumulating with a positive literature trend. This article does not replace physician consultation; individual outcomes still vary.
1. Why "Shame" Is the Biggest Barrier
Statistics from Taiwan's EDACT (Erectile Dysfunction Diagnosis and Counseling Center) show that among ED patients, only 10% seek medical help, and 75% of diagnosed patients choose not to be treated. A large portion of posts on PTT and Dcard begin with "asking for a friend" — reflecting significant resistance to care.
Three major anxieties observed on forums:
- Fear of being recognized: awkwardness in the waiting area and from nursing staff coming in and out of the treatment room
- Fear of being upsold: difficulty distinguishing medical recommendations from commercial pitches
- Fear of not being able to tell one's partner: partner pressure is the most common push toward care, but bringing it up is extraordinarily difficult
Liusmed Clinic's response isn't a "privacy slogan" — it's an executable SOP: the treatment-room-clear protocol (see Section 6).
2. Low-Intensity Shockwave (LI-SWT): What the EAU Guideline Says
2.1 Guideline Position
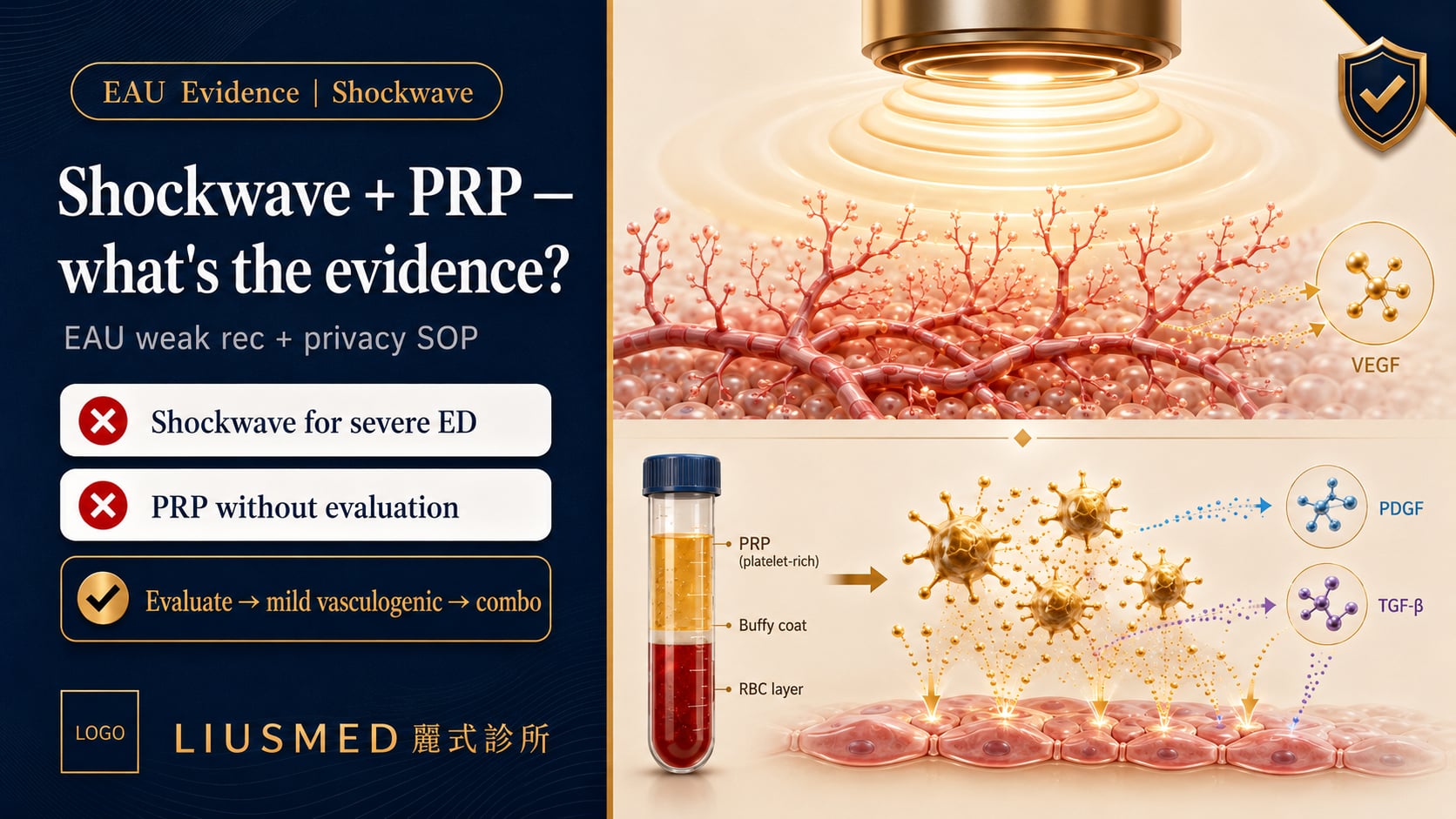
The European Association of Urology (EAU — European urology medical society), in its Sexual and Reproductive Health guideline, lists LI-SWT as a treatment option for mild vasculogenic ED, with a weak recommendation, requiring:
- Full disclosure to patients that "evidence is still accumulating"
- Case-by-case evaluation rather than fixed packages
- Avoid LI-SWT as monotherapy for severe or psychogenic ED
2.2 What Systematic Reviews Say
Campbell JD et al., in Translational Andrology and Urology (2019), synthesized multiple LI-SWT randomized controlled trials (RCTs — gold-standard treatment comparison studies) and concluded:
LI-SWT may bring IIEF-5 score improvement in mild vasculogenic ED, but energy density, pulse count, protocol cadence, and probe shape vary significantly across clinical trials — no standardized protocol has emerged.
Another review, by Chung E & Wang J in Expert Review of Medical Devices (2021), added a critical clinical fact:
Pain is one of the practical factors clinically limiting energy escalation.
This statement supports our "comfort → complete the protocol" logic. Taiwan's own cohort study (Tzou 2021) confirmed significant improvement after completing 12 full sessions — the key is enabling patients to finish the full course comfortably.
2.3 Reasonable Patient Expectations
Based on this evidence, reasonable expectations are:
- Meaningful improvement in most patients, tracked objectively with IIEF-5
- Taiwan clinical average satisfaction ~75%
- Effect can be maintained over 12+ months; booster sessions are available if needed
- Best used alongside physician evaluation — severe ED may need combination approaches
3. PRP Injection: Research Status and Our Clinical Use
3.1 International and Taiwan Research Progress
Evidence for PRP in ED is steadily accumulating. International small-scale RCTs (e.g., Poulios E et al., Journal of Sexual Medicine, 2021) show that PRP can produce mild IIEF improvement over placebo, with a positive literature trend. EAU currently lists PRP as an investigational option — meaning mainstream guidelines are still observing larger trials.
Liusmed Clinic's stance:
- PRP is offered as a shockwave enhancement option, with the physician deciding whether to combine them case by case
- Preparation parameters, injection layers, and doses are transparently documented for traceable, comparable quality
- We track each patient's improvement objectively via IIEF-5
3.2 Painless Shockwave · Near-Painless PRP
- Refined buffering: local anesthesia combined with a refined buffering technique for a near-painless injection experience
- Clinical patient feedback: most patients describe it as "barely noticeable"; a few may see transient bruising that typically resolves within 24–48 hours
- Low-intensity shockwave is painless itself: standard Taiwan medical-education phrasing, no anesthesia required
Why does near-painless delivery matter? A comfortable injection experience lets you complete the full protocol with confidence — and protocol completion is the practical key to outcomes, which is the foundational logic of our third advantage.
4. The "Triangle" Causal Chain
Liusmed Clinic's three differentiating advantages form a single narrative:
Treatment-room clear (privacy)
↓
Low-discomfort PRP (body relaxation)
↓
Complete the protocol (per physician-planned pulses / doses)
↓
Obtain the improvement that research suggests is possible
Key clarification: this causal chain describes process quality — not a claim that "privacy / painlessness = better efficacy." Efficacy still depends on each patient's vascular, neurological, and endocrine status, and on clinical judgment.
5. Who Is Suitable? Who Is Not?
5.1 Potentially Suitable
- Mild to moderate vasculogenic ED
- Unwilling to rely long-term on oral medications, or with contraindications
- Partner relationship affected by sexual performance, willing to evaluate jointly
- Mixed stress-type presentation and vasculogenic factors
5.2 Not Suitable (Contraindications)
- Severe coagulopathy or on anticoagulants
- Active infection in the treatment area
- Penile implant, active Peyronie's disease, chronic corporal pathology
- Active malignancy
- Assessed as purely psychogenic ED (psychological medical intervention is primary)
Important: any assessment must be synthesized by a physician based on history, IIEF-5, and necessary vascular and endocrine investigations. Online self-assessment checklists do not replace clinical evaluation.
6. Treatment-Room Privacy SOP
This is our most specific privacy commitment. A precise distinction is needed:
"Treatment-room clear" ≠ "whole-clinic clear"
We don't shut down the entire clinic — we ensure, for your treatment room specifically:
6.1 Three-Stage Protocol
-
LINE anonymous consultation: ask 3 questions anonymously via LINE — no real name or ID required. After determining suitability, decide whether to schedule.
-
Independent on-site flow: upon arrival at the appointment time, directly enter the consulting room without passing through general waiting areas — minimizing encounters with other patients.
-
Treatment-room clear: during evaluation and treatment, only the male physician is in the treatment room performing the procedure; no nursing staff enter the room. Other clinic services run in parallel.
6.2 Why Not Shut Down the Whole Clinic?
This is an honest trade-off:
- Whole-clinic shutdown affects other patients' access to care — not consistent with medical ethics
- Treatment-room-level clearing already addresses the core anxiety of "having a third party present during the procedure"
- Keeping the clinic operational lets us maintain medical quality and emergency response capability
6.3 VIP Appointment Windows
For patients wanting additional privacy protection (e.g., full buffer times before and after), VIP appointments are available. The VIP premium reflects the extra staff and flow arrangements; we disclose this transparently at booking — no forced upgrade.
7. Treatment Flow (Five Stages)
| Stage | Content | Time |
|---|---|---|
| 1. LINE anonymous consultation | 3 questions without real name | Reply within 1–2 days |
| 2. Outpatient evaluation | History, IIEF-5, BP / lipids / glucose, testosterone if needed | Depends on evaluation |
| 3. Treatment-room-clear scheduling | Reserve dedicated appointment, independent flow | As available |
| 4. Treatment | Shockwave (per evaluation) + PRP (if applicable) | 15–30 minutes |
| 5. IIEF-5 follow-up | Adjust cadence per physician | Every 4 weeks |
Important: not every patient needs PRP combined. Whether to combine, how, and at what dose — physician decision based on evaluation — not upsold.
8. Transparent Pricing
| Item | Price | Notes |
|---|---|---|
| First-visit evaluation (incl. IIEF-5) | Disclosed case-by-case | Includes history + scale |
| Low-intensity shockwave per session | Disclosed case-by-case | Varies with session count / package |
| PRP injection per session | Disclosed case-by-case | Preparation / dose per symptoms |
| VIP treatment-room-clear | Disclosed case-by-case | Reflects staff and flow arrangements |
Exact fees and treatment plans are discussed case-by-case via LINE or in person.
Pricing principles:
- Transparent — all items explained at evaluation
- No coerced course packages — sessions proceed one at a time per physician evaluation
- No "limited-time offer" marketing — consistent with Taiwan medical advertising regulations
9. Risks and Side Effects
9.1 Shockwave
- Common: transient treatment-site soreness, mild skin redness
- Rare: subcutaneous capillary rupture (bruising)
- Very rare: no clearly reported serious adverse events
9.2 PRP Injection
- Common: transient injection-site pain, pinpoint bleeding, bruising
- Occasional: local swelling at injection site for 1–2 days
- Very rare: allergic reaction, infection (under strict sterile operation)
9.3 Shared Contraindications
Already listed in Section 5. If any contraindication is found at evaluation, we decline the procedure and recommend alternatives — we don't take risks for revenue.
10. Ten Commonly Asked Questions
Q1. Does shockwave hurt? Most describe it as "achy or tingling" — intensity is adjusted to tolerance by the physician. Individual experience varies.
Q2. Does PRP hurt? Local anesthesia + buffering technique reduces sharp pain; a 27G needle can still cause transient discomfort or bruising.
Q3. How many sessions are needed? Shockwave commonly uses 6 sessions as a baseline (weekly or biweekly). PRP count is physician-judged — not upsold.
Q4. How long do effects last? Outcomes vary individually; not permanent. Track with IIEF-5 — no specific duration is promised.
Q5. Does it affect fertility? Current literature shows no clear impact. Inform us at evaluation if planning a pregnancy.
Q6. When can I exercise or have sex after treatment? Generally avoid vigorous exercise and sexual activity for 24–72 hours — follow clinic-specific post-treatment instructions.
Q7. Is it suitable for vasculogenic or psychogenic ED? EAU lists LI-SWT as an option for mild vasculogenic ED (weak recommendation). Psychogenic ED requires additional interventions.
Q8. Can I book without giving my real name? You can ask 3 anonymous questions via LINE. On-site visits still require minimum identification and medical records to comply with regulations.
Q9. Can my partner consult with me? Yes. We offer a "joint partner consultation" option — it helps both sides understand the treatment content and expectations.
Q10. Does higher energy mean better results? Not necessarily. Our logic is "comfort → complete the full protocol"; parameters are physician-adjusted within safe limits for your comfort. Taiwan cohort data (Tzou 2021) confirm significant improvement after completing 12 full sessions — protocol completion matters more than raw intensity.
Conclusion: Process as the Anchor, Evidence as the Boundary
The male intimate regeneration field has two extremes — on one side, the avoidance that causes delayed care; on the other, the overclaims of aggressive marketing. Liusmed Clinic chooses the middle path — trading process quality for trust, and evidence limitations for honesty.
Treatment-room clear, low-discomfort PRP, complete-the-protocol — these three pillars don't constitute an efficacy promise; they form a service protocol that is executable, verifiable, and optimizable. As for efficacy itself — your body and research evidence decide that together.
If you have any questions or want to learn more, you can ask 3 anonymous questions via LINE. We won't record your real name until you decide to book an in-person evaluation.
References
- Salonia A, et al. EAU Guidelines on Sexual and Reproductive Health — Erectile Dysfunction. European Association of Urology, 2024. https://uroweb.org/guidelines/sexual-and-reproductive-health
- Campbell JD, et al. Systematic review of low-intensity extracorporeal shock wave therapy for erectile dysfunction. Translational Andrology and Urology, 2019. PMID: 31807437
- Chung E, Wang J. A state-of-art review of low intensity extracorporeal shock wave therapy and lithotripter machines for the treatment of erectile dysfunction. Expert Review of Medical Devices, 2021. PMID: 33583307
- EDACT (Taiwan Erectile Dysfunction Diagnosis and Counseling Center) — prevalence and care-seeking statistics.
Medical Disclaimer
This article is for health education reference only and does not replace physician evaluation. All treatment decisions should rest on individual physician assessment, informed consent, and shared decision-making. Outcomes vary individually and no specific result can be guaranteed.
Related Services

Specialties
Credentials
- Kaohsiung Medical University, School of Medicine
- Attending Physician, Dermatology, Kaohsiung Chang Gung Memorial Hospital
- Attending Physician, Aesthetic Center, Kaohsiung Chang Gung Memorial Hospital
- Visiting Physician, Dermatology, Xiamen Chang Gung Hospital
- Visiting Physician, Aesthetic Center, Xiamen Chang Gung Hospital
"For every surgery, I strive to achieve a good outcome through a small incision and refined technique. Minimally invasive surgery is not just a technique — it's a commitment of respect to every patient."
Want to learn more?
Schedule a consultation for professional evaluation and advice