PRP After Hair Transplant: Better Follicle Survival?
One-Minute Summary
Key Conclusions:
- 2025 systematic review (3 studies, 217 patients): PRP (Platelet-Rich Plasma — concentrate of your own blood platelets rich in growth factors) adjunct significantly improves follicle survival and density.
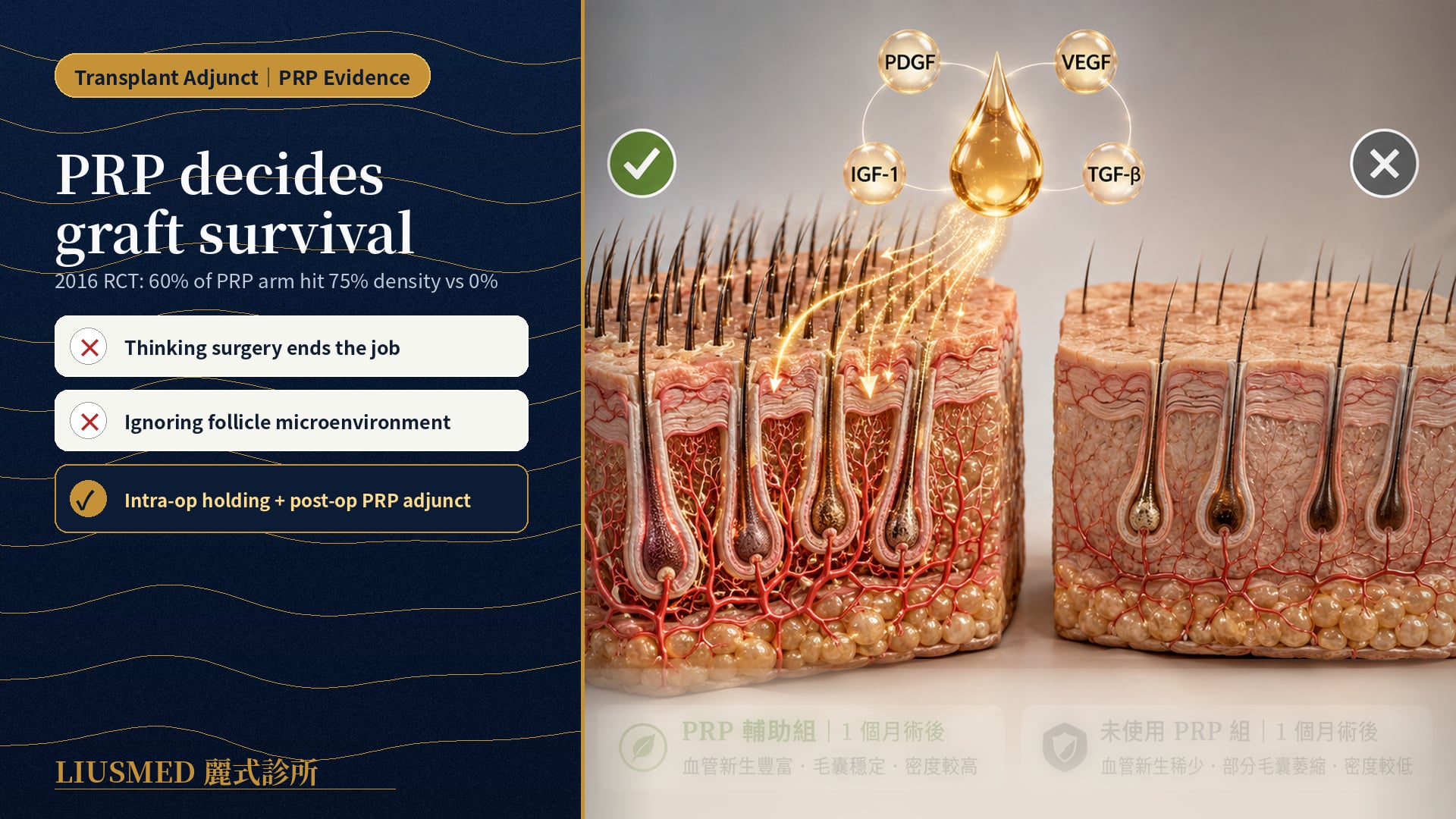
- Landmark 2016 RCT (Randomized Controlled Trial — gold-standard treatment comparison study): at 1 month, 60% of PRP-arm patients achieved >75% density vs 0% in controls (P < 0.001).
- PRP can intervene at three timepoints: (1) intra-op as holding solution; (2) recipient site preparation pre-op; (3) post-op adjunct to accelerate recovery.
- PRP is rich in PDGF (Platelet-Derived Growth Factor), VEGF (Vascular Endothelial Growth Factor — new blood vessel signal), IGF-1 (Insulin-like Growth Factor 1 — growth/repair signal molecule), TGF-β (Transforming Growth Factor Beta — fibrosis & repair signal) growth factors — driving angiogenesis and follicular stem cell activation.
- Clinical takeaway: Not every patient needs PRP, but it is most valuable for patients with large grafts, poor scalp microenvironment, or ongoing AGA (Androgenetic Alopecia — male-pattern hair loss) activity.
Why Transplant Outcomes Sometimes Disappoint
The most common reason for transplant disappointment is not "poor technique" but incomplete follicle survival. A successful transplant should achieve 85–95% survival — but with poor microenvironment, this can drop to 60–70%, leaving density below expectations.
PRP (autologous platelet-rich plasma) targets exactly this variable: follicle survival.
Key insight: PRP is not a "transplant alternative" or "miracle regenerative." It is a precision adjunct for survival optimization — most valuable in large-graft cases or compromised microenvironments.
The Science of PRP
What PRP Contains
The platelet-rich layer extracted by centrifugation contains:
- PDGF (Platelet-Derived Growth Factor): drives fibroblast proliferation and tissue regeneration
- VEGF (Vascular Endothelial Growth Factor): stimulates new vessel formation — critical for follicle survival
- IGF-1 (Insulin-like Growth Factor): promotes follicle cell proliferation and prolongs anagen
- TGF-β (Transforming Growth Factor): regulates tissue repair
- EGF (Epidermal Growth Factor): accelerates epidermal healing
Mechanisms on Follicles
- Accelerated revascularization — transplanted follicles depend entirely on recipient vessels; VEGF speeds this
- Reduced inflammation — excess inflammation damages newly transplanted follicles
- Follicular stem cell activation — enhances bulge stem cell activity
- Anagen prolongation — via IGF-1 pathway
Three PRP Intervention Timepoints
Timepoint 1: Intra-op as Holding Solution
Mechanism: Follicles wait 30 min to several hours between extraction and implantation in holding solution. Saline or proprietary solutions are traditional — but 2023 research showed adding PRP significantly enhances follicle cell viability.
2023 RCT evidence: From 10 AGA patients, 45 follicles each were randomized into 8 holding conditions for 7 days. PRP-supplemented holding solution showed significantly higher CK15 (stem cell marker) than non-PRP.
Clinical implication: Especially valuable for high-volume cases (>2000 grafts) with long surgical times.
Timepoint 2: Recipient Site Pre-op Preparation (4–8 weeks pre-op)
Mechanism: Inject PRP into the recipient site before implantation, optimizing the microenvironment (vascular density, growth factors, oxidative stress) so follicles "land in good soil" when implanted.
Indications:
- Atrophic recipient scalp with poor circulation
- Failed prior transplant requiring re-do
- Severe AGA where the recipient lacks anagen-dominant ratio
Protocol: Typically 1–2 PRP sessions 4–8 weeks before transplant.
Timepoint 3: Post-op Adjunct (Post-op months 1–6)
Mechanism: Accelerate integration between transplanted follicles and recipient vasculature, mitigating shock loss.
Protocol: Typically PRP at 1 month, 3 months, and 6 months post-op.
2016 landmark RCT evidence: This protocol achieved 60% of patients reaching >75% density at 1 month vs 0% in controls (P < 0.001).
Real Differences: With vs Without PRP
| Comparison | Without PRP | With PRP |
|---|---|---|
| Follicle survival | 80–90% | 90–95%+ |
| Patients reaching 75% density at 1 month | 0–20% | 50–60% |
| Post-op shock loss | Moderate | Milder |
| Final outcome (12 months) | Variable | Average slightly superior, better visible density |
| Additional cost | — | +30–50% |
| Additional sessions | — | 3–4 injections pre/post |
Key insight: PRP is not a binary "works or doesn't" question — its evidence shows significant but non-dramatic marginal benefit. For patients pursuing maximal survival and density, PRP is a worthwhile investment; for budget-sensitive patients with healthy native scalp, standard transplant alone can yield satisfactory results.
Who Benefits Most from PRP?
Strongly Recommended
- High-volume grafts (>2500) — long holding times, vascular supply pressure
- Repeat transplants — recipient scarring, compromised microenvironment
- Severe AGA (Norwood IV–V) — poor native follicle microenvironment
- Smokers — impaired microcirculation
- Scarred areas (trauma, surgery, post-radiation)
Marginal Benefit Cases
- Small grafts (<1000) — standard technique reaches high survival
- First-time transplant, healthy scalp, no AGA — already-good microenvironment
- Budget-sensitive — better to invest in surgical precision
PRP Preparation Quality: Critical Variables
Not all PRP is equal. Key parameters:
- Platelet concentration: 1.5–5× baseline blood is optimal; too low is ineffective, too high may even harm
- Leukocyte concentration: scalp PRP prefers leukocyte-poor — reduces inflammation
- Centrifugation: dual-spin (first spin 1000g × 10 min; second 3000g × 5 min)
- Freshness: injection within 30–60 minutes of harvest is optimal
Key insight: Asking about PRP preparation protocol is more important than just "do you offer PRP?" Standardized preparation, fresh injection, and appropriate concentration drive efficacy.
Comparison with Other Adjuncts
| Therapy | Mechanism | Evidence | Indications |
|---|---|---|---|
| PRP | Growth factors + microenvironment | Strong (multiple RCTs) | Survival + accelerated recovery |
| Exosomes | Extracellular vesicle delivery | Moderate (emerging) | PRP non-responders |
| LLLT | Photobiomodulation | Moderate | Long-term maintenance |
| Post-op Minoxidil | Anagen prolongation | Strong | Native hair preservation |
| Post-op Finasteride | DHT reduction | Strong | Prevent native hair recession |
The optimal stack is "Finasteride + Minoxidil + PRP" providing complete "survival + maintenance + microenvironment" coverage.
Side Effects and Risks
PRP from autologous blood does not cause rejection or allergy, but minor risks remain:
- Transient redness/swelling at injection site (24–48 hours)
- Mild pain or scalp tightness
- Rare lightheadedness (related to blood draw volume)
Contraindications:
- Platelet function disorders
- Active infection
- Anticoagulant use (consult primary physician)
- Some autoimmune conditions
Common questions
Do I have to add PRP to my transplant?
Not everyone needs it. PRP tends to help more when the graft count is high, the scalp microenvironment is poor, or androgenetic alopecia is still active. If you're having a small transplant on a healthy scalp with no active hair loss, a standard transplant usually gives a good result on its own — it's worth letting the surgeon judge based on your scalp.
When is PRP done — before or after surgery?
It can actually go in at any of three points. During surgery it can be used as the holding solution for the grafts; 4 to 8 weeks beforehand it can be injected into the recipient area to prime the scalp; and after surgery it's often repeated at months 1, 3, and 6 to help recovery. Which timing, and how many sessions, depends on your situation.
How much difference does adding PRP really make?
There is a difference, but it's more about nudging survival a bit higher and making post-op shedding milder — not a night-and-day change. In the studies, the PRP groups did show better follicle survival and early density. Whether that marginal gain is worth the extra time and cost is something to weigh with your physician.
Is PRP safe? Could I be allergic to it?
PRP is spun down from your own blood, so there's no rejection or allergy to worry about. Most people get at most some short-lived redness or swelling at the injection sites for a day or two, or mild soreness; a few feel lightheaded after the blood draw. That said, if you have a platelet disorder, an active infection, or take blood thinners, check with the doctor first.
Is the PRP the same at every clinic?
Not really. Platelet concentration, how leukocyte-rich it is, the spin protocol, and how fresh it is when injected all affect the result. So rather than just asking whether a clinic offers PRP, it's more useful to ask how they actually prepare it.
Conclusion: PRP Is a Strategic Tool, Not a Must
The core of transplant success remains precise harvest and implantation technique. PRP is an excellent adjunct, especially for those pursuing maximal survival, accelerated recovery, and improved difficult scalps.
If you are planning a transplant or want to enhance existing results, discuss with your physician:
- Does your case fit the PRP-strongly-recommended group?
- Which timepoint(s) of intervention?
- Can your budget and time accommodate full PRP protocol?
See our post-transplant follicle care or book a consultation.
Medical References
- Efficacy of Platelet-Rich Plasma as an Adjunct to Hair Transplantation: Systematic Review. PMC12506585. 2025.
- Effect of Platelet-Rich Plasma and Other Key Factors on Hair Follicle Preservation. PMC10495071. 2023.
- Outcome of Intra-operative Injected PRP Therapy During FUE Hair Transplant: Prospective Randomized Study. PMC5064679.
- PRP as Intraoperative Holding Solution: Pilot RCT. 2021.
- ISHRS Position Statement on Platelet-Rich Plasma in Hair Transplantation.
Editorial review: Reviewed by Dr. Ta-Ju Liu. Last reviewed 2026-04-27.
Related Services

Specialties
Credentials
- Kaohsiung Medical University, School of Medicine
- Attending Physician, Dermatology, Kaohsiung Chang Gung Memorial Hospital
- Attending Physician, Aesthetic Center, Kaohsiung Chang Gung Memorial Hospital
- Visiting Physician, Dermatology, Xiamen Chang Gung Hospital
- Visiting Physician, Aesthetic Center, Xiamen Chang Gung Hospital
"For every surgery, I strive to achieve a good outcome through a small incision and refined technique. Minimally invasive surgery is not just a technique — it's a commitment of respect to every patient."
Want to learn more?
Schedule a consultation for professional evaluation and advice