Steroid Shots for Filler Lumps: The Tissue Atrophy Risk
The Lump Is Gone, But Now There Is a Dent
"The doctor gave me a steroid injection and the lump did soften, but now that area has sunk in and it looks worse than when the lump was there." This is not an uncommon complaint in our clinic. Patients who originally sought treatment for a filler-related lump find themselves dealing with an even more difficult problem: tissue depression and atrophy.
Corticosteroid injections are indeed powerful anti-inflammatory agents and remain indispensable tools across many medical disciplines. However, when used to treat facial filler complications, the potential risks are frequently underestimated. Subcutaneous fat atrophy, dermal thinning, pigmentary changes—these are not rare side effects but near-certain outcomes when steroids are used excessively or inappropriately.
How Steroids Cause Tissue Atrophy (tissue shrinkage and weakening)
Mechanism of Action
Steroids reduce swelling and firmness by suppressing immune responses and inflammatory processes. The problem is that their action is not precisely targeted at the foreign body reaction around the filler—they affect all tissues in the injection area indiscriminately.
Specifically, corticosteroids:
- Suppress fibroblast activity: Reduce collagen synthesis, leading to dermal thinning
- Promote adipocyte apoptosis: Cause subcutaneous fat atrophy, creating irreversible depressions
- Decrease proteoglycan synthesis: Reduce tissue hydration and elasticity
- Inhibit angiogenesis: Decrease local blood supply, further accelerating tissue atrophy
Timeline of Atrophy
| Time After Injection | Possible Changes | Reversibility |
|---|---|---|
| 1-2 weeks | Local swelling reduction, lump softening | Normal treatment response |
| 2-4 weeks | Mild depression at injection site | Partially reversible |
| 1-3 months | Visible skin depression, pigment changes | Difficult to fully reverse |
| 3-6 months | Severe fat atrophy, paper-thin skin | Mostly irreversible |
| 6+ months | Permanent tissue loss | Irreversible |
Key Insight: Steroid-induced tissue atrophy often does not become apparent until weeks after injection, and once severe fat atrophy occurs, the chances of recovery are extremely low. This delayed presentation makes it difficult for both patients and practitioners to recognize the severity of the problem early on.
Which Facial Areas Are Most Vulnerable?
Different facial regions vary dramatically in subcutaneous fat thickness and tissue structure, and their sensitivity to steroids differs accordingly:
High-Risk Areas
- Periorbital region (tear trough, under-eye): Thinnest skin with minimal subcutaneous fat—extremely susceptible to atrophy and depression
- Temples: Thin fat pads mean steroids can easily create visible hollowing
- Nasal bridge: Skin sits directly over cartilage—atrophy creates irregular contour deformities
Moderate-Risk Areas
- Cheeks (malar region): Although there is more fat, repeated injections can still cause asymmetry
- Nasolabial fold area: Injections may deepen existing creases
Relatively Lower-Risk Areas
- Jawline: Thicker tissue, but caution is still warranted
- Forehead: Relatively abundant soft tissue, though high doses still carry risk
Common Clinical Patterns of Steroid Treatment Failure
Pattern 1: Lump Resolves but Depression Appears
The most typical scenario. Steroids successfully suppress the inflammatory reaction around the filler, and the lump genuinely softens or shrinks. But simultaneously, the surrounding normal fat tissue is destroyed, leaving a depression more conspicuous than the original lump.
Pattern 2: Repeated Injections Create a Vicious Cycle
When the first steroid injection produces unsatisfactory results, the practitioner decides to inject again—a second time, a third, a fourth. Each injection deepens the tissue damage, eventually creating severe, multi-focal areas of atrophy. For more case analysis, see: Skin Atrophy After Steroid Injection for Lumps.
Pattern 3: Inflammation Suppressed but Root Cause Remains
Steroids can temporarily suppress inflammation, but if the lump is fundamentally caused by filler accumulation or encapsulation, anti-inflammatory treatment does not eliminate the root cause. Once the medication wears off, inflammation and swelling often return.
Key Insight: Steroid injection for filler lumps is essentially symptomatic treatment rather than curative treatment—it can reduce swelling and inflammation but cannot eliminate the filler material itself. When the primary cause of the lump is material accumulation rather than inflammation, steroids provide limited benefit while potentially causing additional harm.
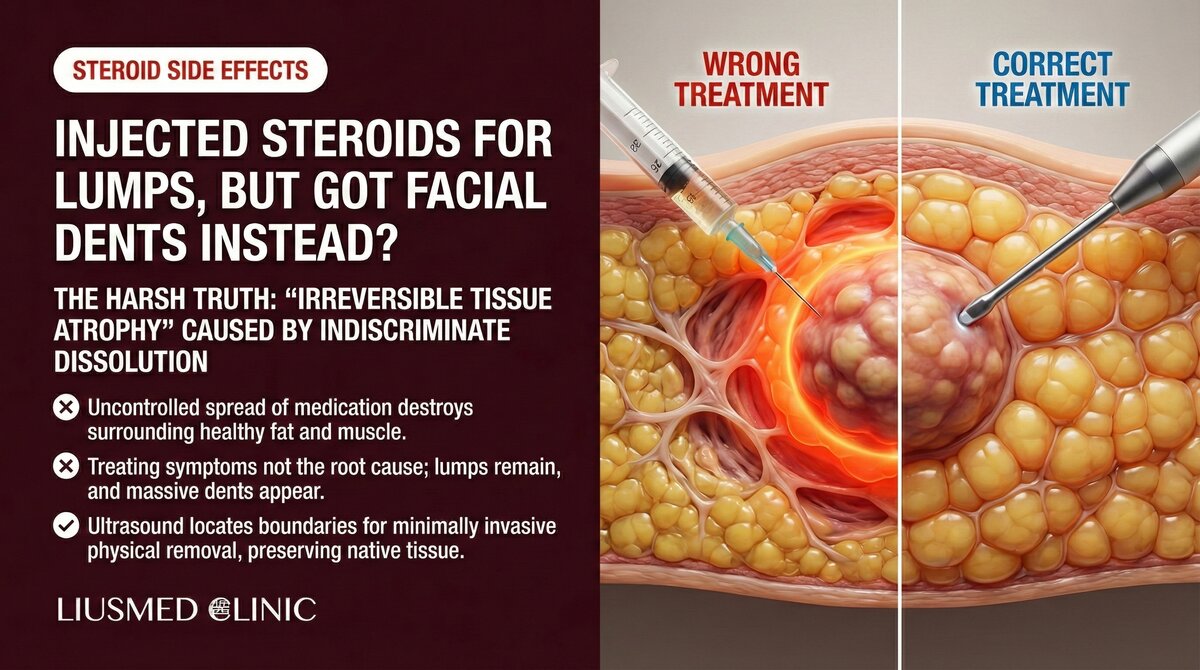
Steroids vs. Ultrasound-Guided Minimally Invasive Extraction
| Comparison | Steroid Injection | Ultrasound-Guided Extraction |
|---|---|---|
| Treatment principle | Suppress inflammation | Directly remove filler |
| Removes filler? | No | Yes |
| Visual guidance | None (blind injection) | Real-time ultrasound |
| Effect on normal tissue | May cause atrophy | Precise operation preserving normal tissue |
| Recurrence risk | High (filler remains) | Low (root removal) |
| Side effects | Fat atrophy, skin depression | Tiny pinhole, rapid recovery |
| Indications | Temporary relief of acute inflammation | Definitive treatment of all filler complications |
Already Have Steroid-Induced Atrophy—Is Recovery Possible?
Steroid-induced tissue atrophy is genuinely difficult to manage, but it is not entirely without options:
Mild Atrophy (Within 2-3 Months Post-Injection)
- Some fat tissue may recover naturally
- Discontinuing steroid injections is the first step
- Patient observation over 6-12 months is necessary
Moderate Atrophy
- Subsequent volume restoration treatments may be needed
- Before any augmentation, the status of the original filler must be confirmed
- Ultrasound evaluation is a critical step
Severe Atrophy
- Tissue reconstruction may require multi-stage treatment
- Autologous fat grafting is a common repair option
- Individualized assessment by an experienced physician is essential
For the specific issue of steroid use with collagen stimulator complications, see: Why Steroid Injections Fail for Sculptra Lumps.
When Are Steroid Injections Still Appropriate?
Steroids are not universally inappropriate. In the following specific scenarios, short-term, low-dose steroid use may be justified:
- Acute allergic reactions: Rapid immune suppression is needed
- Severe acute inflammation: As temporary symptom control while planning definitive treatment
- Post-operative swelling: Very low-dose steroids may help reduce post-extraction swelling
The key principle: steroids should serve as temporary adjuncts, not long-term treatment strategies.
What Is the Correct Treatment Approach?
When facing filler lumps, the ideal treatment process should be:
- Ultrasound evaluation: Confirm material type, location, and degree of encapsulation
- Root cause analysis: Determine the cause of the lump (material accumulation, encapsulation, inflammation, infection)
- Treatment planning: Select the most appropriate treatment based on diagnostic findings
- Definitive treatment: Perform minimally invasive extraction under ultrasound guidance
- Post-treatment follow-up: Ongoing monitoring of recovery
Skipping the evaluation steps and proceeding directly to steroid injection is like prescribing medication without running any diagnostic tests—it may work by chance sometimes, but more often it misses the correct diagnosis and may cause additional harm.
We recommend starting with a comprehensive ultrasound evaluation before deciding on a treatment direction. If you have been considering or have already tried steroid treatment with unsatisfactory results, schedule a consultation so we can provide a more precise assessment and recommendations.
Common questions
Does a steroid shot for a filler lump always cause a dent or atrophy?
Not everyone who gets one ends up with a dent. It really comes down to the dose, how many times it is repeated, and where it goes in. Used short-term, at a low dose, in the right spot, the risk stays manageable. But repeated shots, higher doses, or injections into thin-skinned areas with little fat push the odds of atrophy up a lot. So the question isn't whether it can be used, but how and how often.
Why does the dent show up weeks later instead of right away?
Steroid-related tissue atrophy usually isn't something you see the day of the shot. It tends to surface gradually over a few weeks. That is why the lump softening early on can feel like a good result, and the sinking only becomes obvious later. This delay is a big reason people don't catch the problem early and keep going back for more shots.
Which facial areas are more likely to hollow out after a steroid injection?
The thinner the skin and the less fat underneath, the higher the risk. The under-eye area (tear trough and eye bags) is especially prone, followed by the temples and the nasal bridge. Those spots already have thin tissue, so once atrophy sets in it shows clearly and is harder to deal with. The jawline and forehead have thicker tissue, but higher doses still carry risk there.
If a dent has already formed, can it recover?
It depends on the severity. For mild depressions within the first two to three months, stopping the steroid comes first, and some fat tissue may gradually come back on its own, though it takes time to watch and see. More severe atrophy is trickier — it often means checking with ultrasound whether the original filler is still there before considering options like fat grafting, and that has to be judged case by case by your physician.
So should steroids never be used at all?
Not at all. For an acute allergic reaction, severe acute inflammation, or to ease swelling after a minimally invasive extraction, short-term low-dose use is reasonable. The point is to treat it as a temporary helper, not a repeated long-term fix for a lump. When the lump is really just filler sitting there, calming the inflammation won't address the underlying cause.
Conclusion
Steroids are a double-edged sword. At the right time and in the right dosage, they can be useful adjuncts. But when used repeatedly as a supposed cure-all for filler lumps, the cost can be greater than the original problem. True treatment does not suppress symptoms with medication—it identifies the root cause and addresses it with precision.
Related Services

Specialties
Credentials
- Kaohsiung Medical University, School of Medicine
- Attending Physician, Dermatology, Kaohsiung Chang Gung Memorial Hospital
- Attending Physician, Aesthetic Center, Kaohsiung Chang Gung Memorial Hospital
- Visiting Physician, Dermatology, Xiamen Chang Gung Hospital
- Visiting Physician, Aesthetic Center, Xiamen Chang Gung Hospital
"For every surgery, I strive to achieve a good outcome through a small incision and refined technique. Minimally invasive surgery is not just a technique — it's a commitment of respect to every patient."
Recovery after any procedure needs peer support too
Want to learn more?
Schedule a consultation for professional evaluation and advice