
Fat Grafting Lumps & Calcification
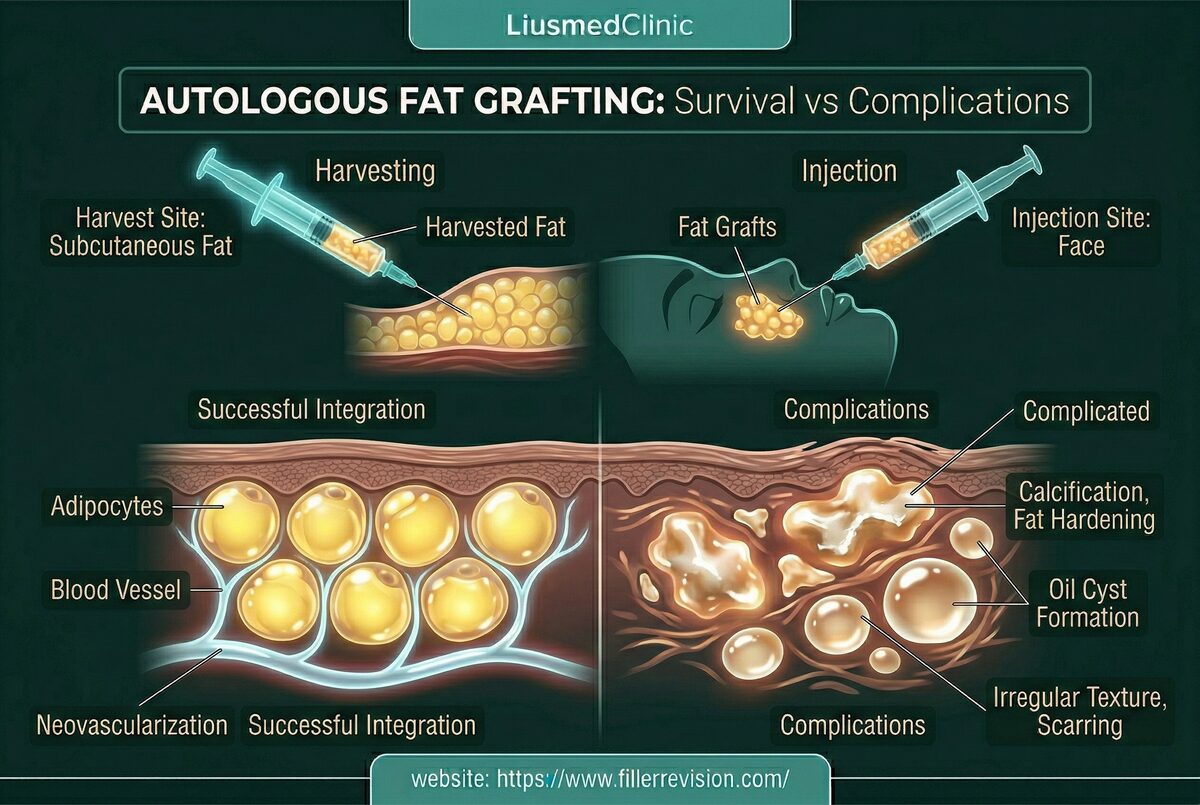
Autologous fat transfer complications occur when injected fat cells fail to establish adequate blood supply and undergo necrosis—cell death that leads to oil cysts, fibrous lumps, or calcified nodules. Studies report palpable lump rates of 5-15% following facial fat grafting. The challenge is that these complications involve the patient's own tissue, making them difficult to distinguish from normal anatomy without imaging. Oil cysts contain liquefied necrotic fat that can persist indefinitely, while calcifications represent the body's attempt to wall off dead tissue with calcium deposits—creating rock-hard masses that mimic tumor on palpation.
Three Core Strengths of Liusmed Revision
Clean Removal
Stubborn masses are removed completely so residual tissue does not keep flaring.
Even Result
After removal the surface stays smooth, without new dents or waviness.
Precise, Not Excessive
Like fat grafting in reverse — the amount and location removed are judged precisely.
Common Symptoms
Fat Necrosis & Calcification Cascade
Fat survival after grafting depends on rapid revascularization—the transferred cells must establish a blood supply within 48-72 hours or they die. Factors that impede this process include over-injection of large boluses (exceeding the tissue's ability to nourish), placement in poorly vascularized areas, rough handling of harvested fat, and individual patient healing response. Dead fat cells rupture, releasing their lipid contents into the surrounding tissue. The body attempts to contain this oil through encapsulation—forming oil cysts. Over months, inflammatory mediators and calcium deposition convert some of these cysts into calcified nodules—rock-hard masses that are indistinguishable from pathological calcifications on imaging and frequently trigger unnecessary cancer workups.
Why Traditional Treatments Fail
Risks of Conventional Surgical Approach
Traditional surgical excision of fat lumps requires incisions that leave visible scars on the face. Conventional liposuction cannulas are designed for body contouring and are too large and aggressive for delicate facial structures—risking nerve damage, uncontrolled volume loss, and contour irregularities (dents). Steroid injections can reduce inflammation around oil cysts but cannot dissolve calcified tissue and risk causing fat atrophy in surrounding healthy fat. Observation is often recommended but is inadequate for symptomatic lesions—calcified nodules will not resolve spontaneously and oil cysts rarely fully absorb.
“The critical first step with fat grafting complications is ultrasound classification—live fat, oil cyst, fibrous lump, or calcification. Each requires a completely different approach, and getting this wrong wastes everyone's time.”
Dr. LiuFour Pathologies, Four Different Treatments
Ultrasound-Guided Pinhole Micro-Extraction
The critical insight with fat grafting complications is that 'a lump' is not a diagnosis. Every palpable abnormality falls into one of four distinct categories — viable fat, oil cyst, fibrous mass, or calcification — and each requires a completely different treatment. Treating all lumps the same way is the most common clinical error.
Your Own Tissue Makes Diagnosis Harder
Unlike synthetic fillers, fat grafting complications involve the patient's own tissue, making visual and tactile assessment unreliable. Imaging-based classification is mandatory, not optional.
Each Pathology Has Its Own Solution
Oil cysts need drainage, calcifications need fragmentation, fibrous masses need dissection. Applying one technique to all four pathologies guarantees suboptimal outcomes.
Preserve What Survived
The healthy fat that successfully established blood supply is stable and valuable. The goal is targeted removal of defective tissue while protecting every viable cell.
Ultrasound-Guided Aspiration & Extraction
Using ultrasound, we first distinguish between viable fat, oil cysts, fibrous lumps, and calcified nodules—each requiring a different treatment approach. Oil cysts are drained via fine-needle aspiration. Calcified masses are mechanically broken down and extracted through micro-cannulas. Fibrous lumps are dissected and aspirated. Throughout, we preserve all healthy surrounding fat to maintain natural facial volume and contours.
Diagnostic Ultrasound Classification
Cyst Drainage
Calcification Breakdown
Micro-Cannula Extraction
Common Questions
Will I lose volume?
Is it permanent?
Why did my fat grafting form lumps?
Can calcified fat lumps be removed without surgery?
How long after fat grafting do lumps appear?
Will removing the lump leave a dent?
My lump showed up on a mammogram/X-ray—should I worry?
Composition, brands, and removability — compiled on our filler-revision specialty site.
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then reach out via the button below with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.