
Multiple Lipomas: 0.5 cm Hidden-Incision Removal
Many lipomas, each shrunk to the smallest possible scar tucked into the skin
Multiple lipomas are usually small (within 1–2 cm). Liusmed removes each one — together with its capsule — through a 0.5 cm (often 0.3 cm) hidden incision, under ultrasound guidance and gentle pain-relief anesthesia, so you never trade lumps for a body full of scars.
Why Choose Liusmed for Multiple Lipomas
Multiple in One Session
Several lipomas are planned for removal in one session, reducing repeated anesthesia and visits.
Minimal Incision Each
Each lipoma is handled through its own minimal incision, balancing clearance with appearance.
Education & Follow-Up
Multiple lipomas reflect an individual tendency and new ones may appear; we explain this honestly and arrange long-term follow-up.
Liusmed 0.5/0.3 cm Hidden Incision + Gentle Pain-Relief Anesthesia
One method, used for both multiple lipomas and multiple steatocystoma. The point is not just a small incision, but removing the lesion together with its capsule through the smallest possible wound.
Ultrasound mapping
High-resolution ultrasound confirms each lesion’s size, depth and nearby vessels and nerves, planning the most hidden incision.
Gentle pain-relief anesthesia
Tumescent local anesthesia with an ultrasound-guided nerve block — patient awake, outpatient, no general anesthesia.
0.5 cm hidden incision
Multiple lipomas are usually within 1–2 cm, so the incision is kept within 0.5 cm — often 0.3 cm — tucked into the skin’s natural lines.
Complete capsule removal
Removing the capsule (the membrane enclosing the lipoma) is what keeps same-site recurrence low; many lesions are staged by priority.
This incision of about a quarter of the lesion diameter applies to selected superficial lesions; deep, fibrous, or vascular lesions may still need a larger incision. We explain this honestly in consultation.

Multiple lipomas sit in the subcutaneous fat layer, with a thin capsule, soft and mobile; the fine surface line illustrates the tiny hidden-incision position.
What are multiple lipomas?
A lipoma is a benign tumor of mature fat cells — the most common soft-tissue tumor — soft, mobile and usually painless. When several occur in the same person, they are called multiple lipomas, favouring the forearms, thighs and trunk.
Familial Multiple Lipomatosis (FML) often shows autosomal dominant inheritance, with an often-cited rough prevalence of about 1 in 50,000. Sporadic multiple lipomas are linked at the molecular level to HMGA2 (a gene associated with lipomas) rearrangements, but the evidence is not yet enough to call HMGA2 the single cause of FML — so we will not state the cause more absolutely than the literature does.
Why isn’t liposuction alone recommended for multiple lipomas?
You will often read that "many lipomas should just be liposuctioned for a small wound." The port is indeed small, but liposuction mainly removes the fatty content while the capsule that encloses the tumor is usually left behind.
The literature reports a roughly 30–40% recurrence rate for liposuction alone — because the retained capsule refills. To keep same-site recurrence low, the key is to remove the capsule too, not just the fat inside.
Liusmed’s 0.5/0.3 cm hidden incision aims to remove the lesion together with its capsule through a tiny wound — low recurrence and minimal scar at once.
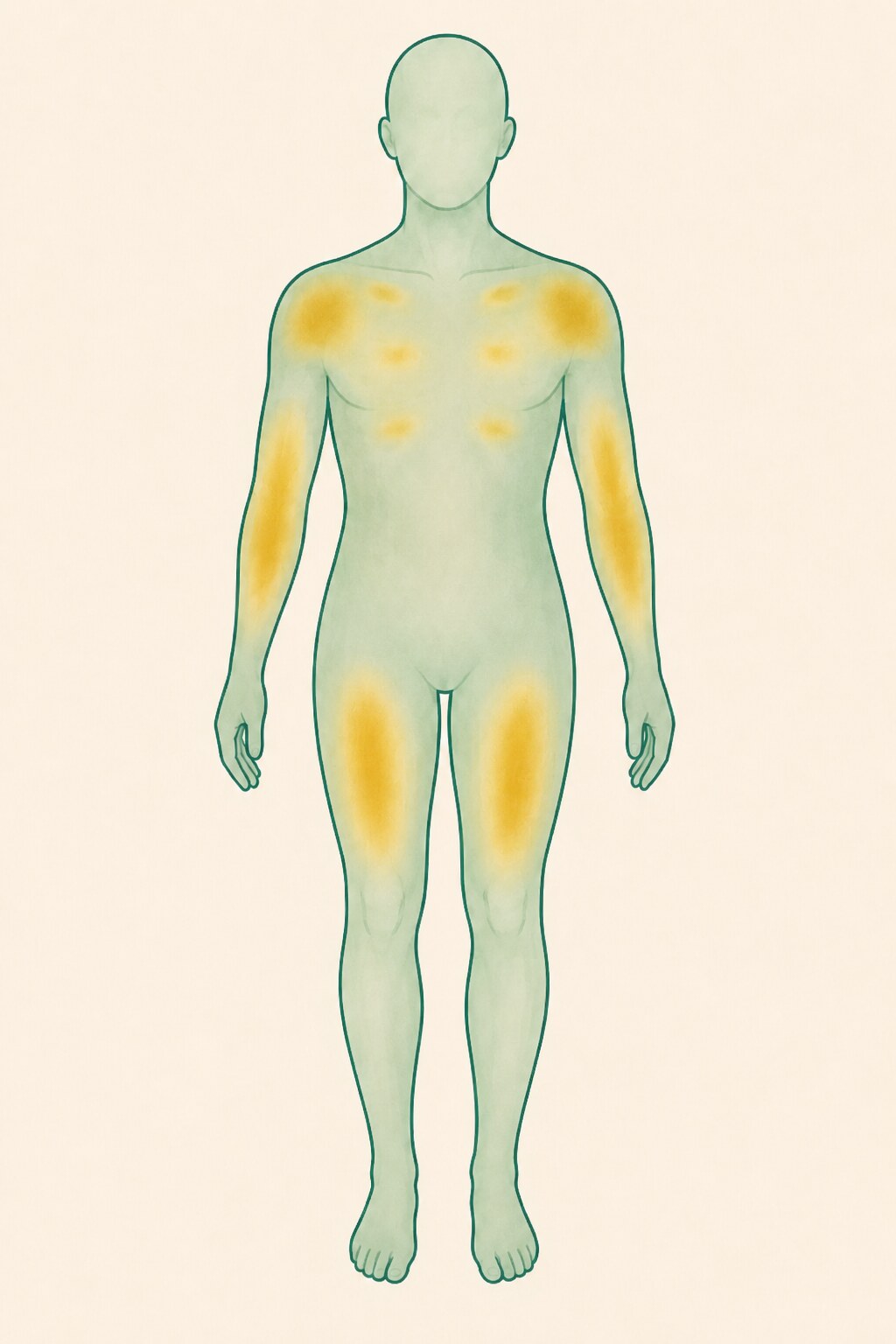
Where do multiple lipomas appear?
Multiple lipomas typically appear on the forearms, thighs and trunk, and less often on the head, neck and shoulders. If the lumps are symmetric around the neck/shoulder girdle, or come with marked pain, conditions such as Madelung disease or Dercum disease must first be excluded (see table) — the approach is completely different.
"Many lumps" are not always multiple lipomas
Separating the look-alikes first determines the right work-up and treatment
| Condition | Key features | Typical distribution |
|---|---|---|
| Familial Multiple Lipomatosis (FML) | Many, painless, encapsulated, mobile | Forearms, thighs, trunk |
| Madelung disease (symmetric lipomatosis) | Symmetric, diffuse, non-encapsulated deposits | Neck, shoulder girdle, upper back |
| Dercum disease (adiposis dolorosa) | Pain-predominant, often with fatigue | Abdomen, inner limbs |
| Gardner syndrome | With bowel polyps, osteomas, epidermal cysts | Trunk, limbs (check family colon-cancer history) |
| Angiolipoma | Often tender, contains vascular elements | Forearms, trunk |
| Atypical lipomatous tumor / liposarcoma | Deep, firm, rapidly enlarging, fixed | Deep, lower limbs (needs imaging) |
When should you be cautious and image first?
A typical lipoma rarely turns malignant; the real priority is not to mistake a tumor that was never a simple lipoma for one. With any of the following, we recommend high-resolution ultrasound first, and MRI or biopsy if needed:
- A superficial lump over 10 cm, or a deep (subfascial/intramuscular) one over 5 cm
- Rapid enlargement over a short time
- Becoming firm, fixed, no longer mobile
- Unexplained pain
- Thick septa or atypical features on imaging
"See it to treat it safely" — ultrasound is valuable, but it cannot fully replace MRI or biopsy for atypical lesions; we judge honestly per lesion.
How are many lesions scheduled?
For multiple lesions the strategy is not to clear everything at once, but to stage: address painful, compressing, rapidly changing or diagnostically uncertain lesions first, then the most cosmetically troubling areas.
Under gentle pain-relief anesthesia, nearby lesions can be treated in a single outpatient session, the rest staged by recovery. Surgery cannot change the constitution, so new lipomas may still form elsewhere — we help keep every session hidden-scar and low-burden, rather than promising a one-time cure of the tendency.
Frequently Asked Questions
Do all of my multiple lipomas have to be removed?
No. Typical, superficial, painless, long-stable lipomas can be observed; removal is prioritised for painful, compressing, function-limiting, cosmetically distressing or diagnostically uncertain lesions. We map them with ultrasound first.
I read that liposuction is suitable for multiple lipomas — is that true?
Liposuction has a small wound but usually leaves the capsule; the literature reports ~30–40% recurrence for liposuction alone. Liusmed removes each lipoma with its capsule through a 0.5 cm (often 0.3 cm) hidden incision to minimise same-site recurrence.
How is a 0.5/0.3 cm hidden incision possible? Is it painful? General anesthesia?
Multiple lipomas are usually within 1–2 cm, suited to a tiny incision. We work under ultrasound guidance and gentle pain-relief anesthesia, patient awake, outpatient, no general anesthesia, with staging for many. Deep or fibrous lesions may need a larger incision; we explain first.
Can multiple lipomas turn malignant?
A typical lipoma rarely transforms; the priority is not to mistake an atypical lipomatous tumor or liposarcoma for a lipoma. For deep, rapidly enlarging, firm or fixed lesions we arrange ultrasound, and MRI or biopsy if needed.
Will they grow back after removal?
For a single lipoma removed completely with its capsule, same-site recurrence is low. But a multiple-lipoma tendency often produces new ones elsewhere — not recurrence at the same spot — which we manage in staged, scar-minimising sessions.
Book a Multiple-Lipoma Assessment
Dr. Ta-Ju Liu assesses each lesion with ultrasound and plans the hidden-incision, staged approach that suits you.
Book a ConsultationReferences
- Kim DL, Hwang SM, Lee JS, Kim HD, Shin JH. Minimally Invasive Excision of Lipomas Using an Extractor. JAMA Dermatology, 2014. doi:10.1001/jamadermatol.2014.2308
- Lee K, Park S, Kim J. MOTIF Technique for Large Lipoma Removal. Journal of Dermatological Surgery, 2021.