
Steatocystoma Multiplex: 0.5 cm Hidden-Incision Cyst-Wall Removal
Recurring small cysts, cleared one by one with scars tucked into the skin
Steatocystoma multiplex is a sebum-related dermal cyst; medication cannot remove existing cysts, and the key to clearance is removing the cyst wall completely. Liusmed treats each one through a 0.5 cm hidden incision, with ultrasound assistance and gentle pain-relief anesthesia.
Why Choose Liusmed for Steatocystoma Multiplex
Plan Many Together
Depending on number and distribution, we plan to treat many cysts together or across staged sessions.
Minimal, Scar-Aware
We balance clearance with appearance, keeping scars as faint as possible.
Honest Education
This is a genetic tendency and new cysts may form; we explain the expected outcome honestly.
Liusmed 0.5 cm Hidden Incision + Gentle Pain-Relief Anesthesia
The same method as for multiple lipomas. For steatocystoma, "clearance" is not about squeezing out the oil but removing the cyst wall (the source of secretion and regrowth) completely — if any wall remains, the cyst refills and recurs.
Ultrasound differentiation
High-resolution ultrasound helps distinguish steatocystoma from epidermoid cyst and lipoma, and maps each lesion’s depth and extent.
Gentle pain-relief anesthesia
Tumescent local anesthesia with an ultrasound-guided nerve block — patient awake, outpatient, no general anesthesia.
0.5 cm hidden incision
Express the oily sebum through a hidden micro-incision of about 0.5 cm, tucked into the skin’s natural lines.
Complete cyst-wall removal
Extract the entire cyst wall with fine instruments — the key to low same-site recurrence; multiple lesions are staged by site.
No procedure is truly "scarless"; temporary post-inflammatory pigmentation is common and fades over time. Steatocystoma is largely constitutional/genetic — surgery clears existing lesions but cannot stop new ones forming elsewhere.
What is steatocystoma multiplex?
Steatocystoma multiplex (sometimes called multiple sebaceous cysts) is a benign dermal cyst arising from the pilosebaceous unit, containing oily sebum with sebaceous glands in the cyst wall. It usually appears after puberty, is linked to variants in KRT17 (a keratin gene), and may be sporadic or autosomal dominant.
It favours the chest, axillae, upper arms and trunk, typically as flesh-to-yellow soft mobile cysts, usually without an obvious central opening. Most are painless but do not resolve on their own; if the wall ruptures and inflames, it can become the painful, suppurative variant.
A steatocystoma is not an epidermoid cyst — the cross-section shows it best

Left: a steatocystoma connects to a sebaceous gland with oily sebum inside; right: an epidermoid (sebaceous) cyst usually has a surface opening (punctum) and keratin inside. Different origin, different content.
Steatocystoma vs epidermoid (sebaceous) cyst — key differences
| Feature | Steatocystoma multiplex | Epidermoid cyst |
|---|---|---|
| Origin | Pilosebaceous unit | Epidermis / follicular infundibulum |
| Content | Oily sebum | Keratin debris |
| Central punctum | Usually absent | Often present |
| Common sites | Chest, axillae, upper arms | Face, neck, trunk |
| Key to clearance | Remove the cyst wall completely | Remove the cyst sac completely |
"Leave it alone" is not the only answer: definitive vs palliative
You will often read that "for multiple sebaceous cysts, no treatment is the best treatment" — understandable if you want to avoid surgery and many scars, but it is not the only option.
The key is to separate treatments into definitive (truly clearing existing cysts by removing the wall) and palliative (temporary relief only). Squeezing, needle drainage, or medication alone leaves the wall behind, so recurrence is to be expected.
Where each option stands (an honest layering)
| Approach | Clears existing cyst? | Note |
|---|---|---|
| Micro-incision complete cyst-wall removal | Yes (definitive) | 0.5 cm hidden incision, gentle pain-relief anesthesia — our mainstay |
| CO2 laser ablation + wall removal | Close to definitive (if wall removed) | Can shorten total scar length when there are many lesions |
| Oral isotretinoin | No | Lowers sebum and inflammation, helps the inflammatory variant, does not remove the wall |
| Needle aspiration / squeezing | No | High recurrence; squeezing may trigger the suppurative variant |
| Cryotherapy | Often unreliable | Scarring and pigment change, inconsistent results |
This is why Liusmed emphasises "cleared by surgery" — removing the cyst wall completely through a 0.5 cm hidden incision, for low recurrence and minimal scar; the inflammatory variant is first calmed, then treated.
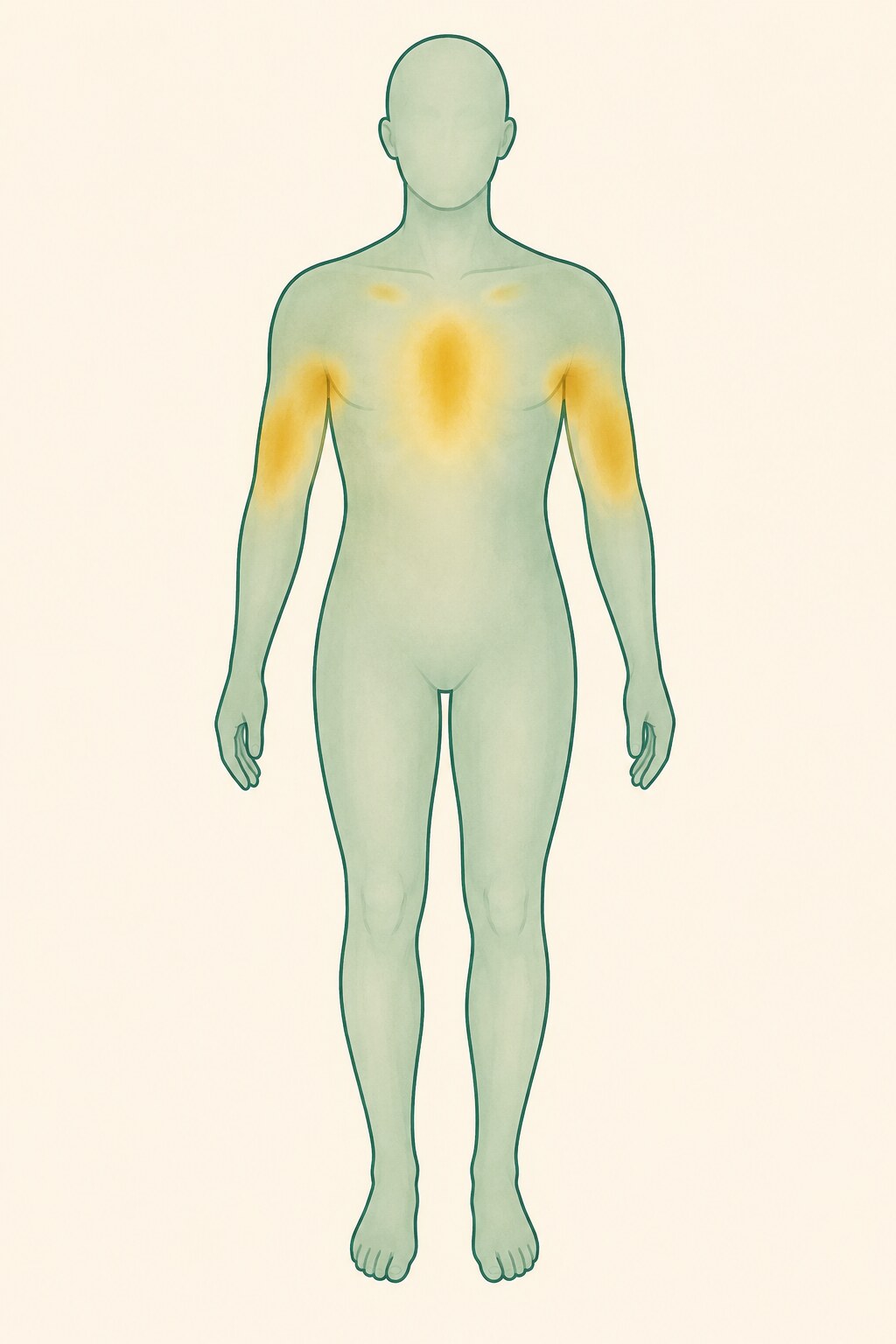
Where does steatocystoma multiplex appear?
Steatocystoma arises where sebaceous glands are dense, so it most commonly appears on the chest (sternal area), axillae and upper arms, then the trunk and abdomen, and less often the face, scalp or groin. The distribution essentially mirrors the body’s sebaceous-gland map.
Many cysts, or already inflamed — how is it scheduled?
For many lesions we stage: address the most cosmetically troubling or already-inflamed ones first, the rest by site and recovery. Under gentle pain-relief anesthesia, nearby lesions can be treated in a single outpatient session.
If it is already the suppurative variant (red, painful, draining, sinus tracts), we first calm the inflammation and pain (oral antibiotics, isotretinoin, drainage if needed), then remove the remaining cyst walls once stable.
Frequently Asked Questions
Is multiple steatocystoma the same as a common "sebaceous cyst"?
Not exactly. A common "sebaceous cyst" is mostly an epidermoid cyst — keratin content, often a surface punctum. A steatocystoma is sebaceous-related — oily sebum, sebaceous glands in the wall, usually no punctum. Different origin and content.
Can oral isotretinoin cure it?
Not a cure. It lowers sebum and inflammation, helps the inflammatory variant and may shrink some cysts, but cannot remove the existing wall, which usually refills after stopping. Clearing an existing cyst requires removing the wall completely.
Can it be completely scarless and cured all over in one go?
We remove the wall through a 0.5 cm hidden incision so scars can be very small and hidden, but nothing is truly "scarless"; temporary pigmentation is common. It is largely constitutional, so surgery clears existing lesions but cannot stop new ones — hence staging.
Is it painful? Do I need general anesthesia?
No general anesthesia. We work with ultrasound assistance under gentle pain-relief anesthesia, patient awake, outpatient; many cysts in one session or staged, balancing cosmesis and comfort.
Can I just squeeze or drain them?
Not advisable. There is no opening to the surface; squeezing or needle drainage only expels oil while the wall remains, so recurrence is high — and squeezing may rupture the wall and trigger the painful suppurative variant. The correct approach removes the wall completely.
Book a Steatocystoma Assessment
Dr. Ta-Ju Liu differentiates and assesses each lesion with ultrasound, planning the hidden-incision, staged clearance that suits you.
Book a Consultation