
Biofilms & Chronic Infection
Biofilm-associated filler infections represent one of the most misdiagnosed and undertreated complications in aesthetic medicine. Bacteria colonize the filler surface and form organized communities protected by an extracellular polysaccharide matrix (the biofilm) that renders them 100-1000x more resistant to antibiotics than free-floating bacteria. Published literature reports biofilm infection rates of 0.5-2% across all filler types, with permanent fillers carrying the highest long-term risk. These infections can remain dormant for months or years before flaring, and the cyclical pattern of improvement with antibiotics followed by relapse is the hallmark clinical signature. Without removing the filler substrate that the biofilm lives on, cure is impossible.
Three Core Strengths of Liusmed Revision
Clean Removal
Stubborn masses are removed completely so residual tissue does not keep flaring.
Even Result
After removal the surface stays smooth, without new dents or waviness.
Precise, Not Excessive
Like fat grafting in reverse — the amount and location removed are judged precisely.
Common Symptoms
The Biofilm Fortress
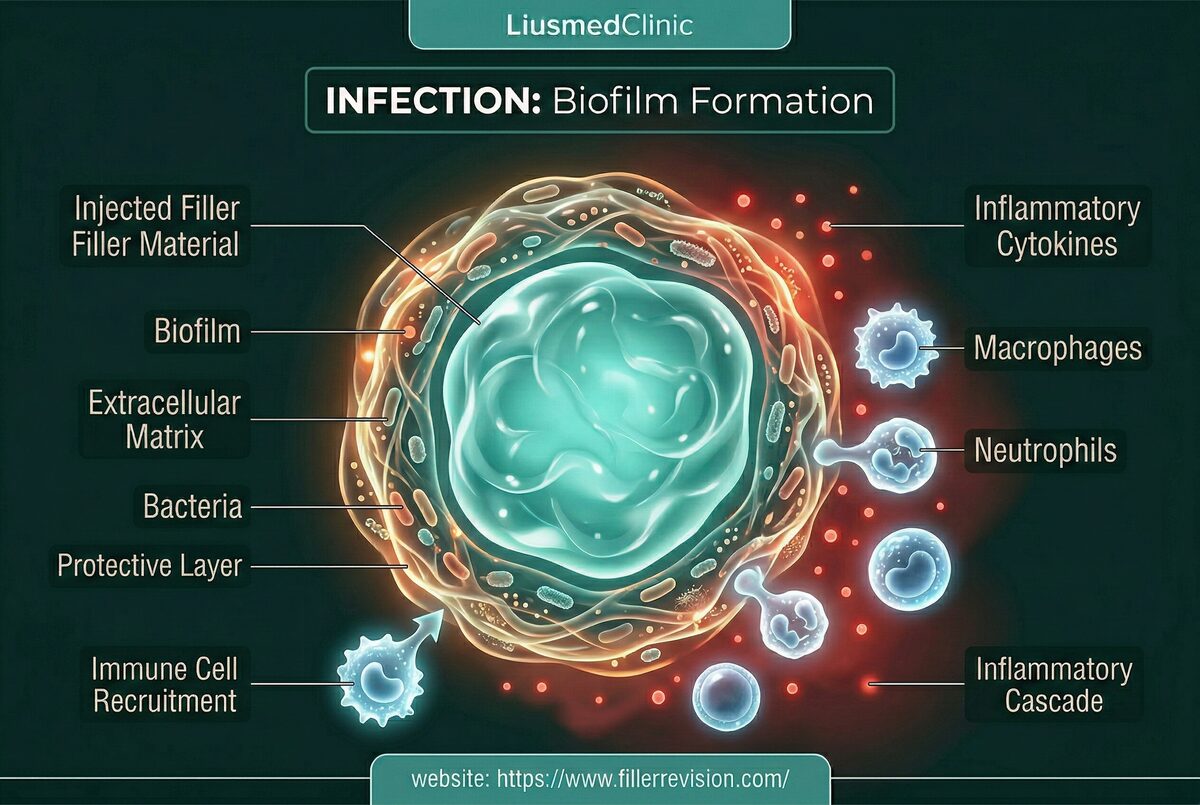
Biofilm formation is a fundamental survival strategy of bacteria. When bacteria encounter a foreign body surface (the filler), they adhere, multiply, and secrete a protective extracellular matrix—the biofilm. Within this structured community, bacteria exist in a dormant, metabolically inactive state that makes them virtually impervious to antibiotics, which target actively-growing bacteria. The biofilm can form from bacteria introduced during the original injection, from transient bacteremia during dental work, or from hematogenous seeding during any systemic infection. Once established, the biofilm cycles between dormancy and periodic release of planktonic (free-floating) bacteria into surrounding tissue—causing the characteristic flare-up pattern. Each flare activates the immune response, causing swelling and inflammation, while the biofilm reservoir remains untouched.
Why Traditional Treatments Fail
Why Antibiotics Cannot Cure Biofilm Infections
Oral and intravenous antibiotics are effective against planktonic bacteria released from the biofilm into surrounding tissue—explaining why patients experience temporary improvement during antibiotic courses. However, the biofilm community on the filler surface is protected by its extracellular matrix, which blocks antibiotic penetration and contains bacteria in a metabolically dormant state that antibiotics cannot target. When antibiotics are discontinued, the biofilm resumes releasing bacteria, and symptoms return within weeks to months. This cycle—improvement with antibiotics, relapse after stopping—can continue indefinitely. Long-term antibiotic use carries its own risks: antibiotic resistance development, gut microbiome disruption, and organ toxicity. The only definitive treatment is removing the foreign body substrate the biofilm colonizes.
“A biofilm infection is like a termite colony inside a wall—you can spray the ones that come out, but until you remove their nest, they'll keep coming back. The filler IS the nest.”
Dr. LiuYou Can't Sterilize What You Don't Remove
Ultrasound-Guided Pinhole Micro-Extraction
The defining feature of biofilm infections is that the filler itself is the problem. The biofilm doesn't just happen to be on the filler — the filler IS its home. As long as that home exists, antibiotics will only ever provide temporary relief. Cure requires removing the substrate, not just fighting the bacteria.
The Filler IS the Biofilm's Home
Bacteria form biofilms specifically on foreign body surfaces. The filler provides the structural scaffold the biofilm needs to survive. Remove the scaffold, and the biofilm cannot persist.
Antibiotics Suppress, They Never Cure
Each antibiotic course kills the free-floating bacteria released by the biofilm, providing temporary improvement. But the biofilm colony on the filler surface is protected and will reactivate indefinitely.
Culture-Guided Therapy Replaces Guesswork
Empiric broad-spectrum antibiotics are a shotgun approach. Sending extracted material for culture identifies the exact organism, enabling targeted therapy that is more effective and less disruptive.
Source Elimination & Targeted Irrigation
Curing a biofilm infection requires removing its home—the colonized filler material. We extract the infected filler through pinhole entries under ultrasound guidance, then perform pulse lavage irrigation of the tissue pocket to mechanically disrupt any residual biofilm. Tissue samples are sent for culture and sensitivity testing to guide targeted post-procedure antibiotic therapy. This source-elimination approach converts an incurable chronic infection into a treatable acute condition.
Infected Filler Extraction
Pulse Lavage Irrigation
Culture & Sensitivity Testing
Culture-Guided Targeted Antibiotics
Common Questions
Can filler infection happen years later?
How do you know it is a biofilm and not just inflammation?
Will antibiotics alone cure a filler biofilm?
Is it dangerous if left untreated?
Can I reinject filler after the infection is cleared?
Is the swelling from infection or from the filler itself?
How do you prevent reinfection during the removal procedure?
Posted in the forum? We can help expedite your appointment.
Standard booking takes 3+ months. If you post your case in the FillerRescue forum first and then reach out via the button below with the required info, we’ll watch for earlier slots and help arrange your appointment as soon as possible.