Why Does Calcification Occur After Fat Grafting? The Science of Fat Survival and Hard Lump Formation
Autologous Fat: Natural Does Not Mean Risk-Free
Autologous fat grafting is often considered the most "natural" filling method because it uses the patient's own tissue. However, a natural source does not guarantee a natural outcome. The survival rate of grafted fat is never 100%, and the fat that does not survive is where problems begin.
When fat cells cannot establish adequate blood supply in their new environment and die, the body must process this necrotic tissue. The outcome may be harmless absorption, but it can also be oil cysts, fibrous encapsulation, or — most troublingly — calcification.
Key Insight: The core challenge of autologous fat grafting is not the "injection" itself but "survival." Grafted fat survival rates typically range from 30-70%, meaning a significant proportion of fat cells will die after transplantation. The fate of necrotic fat — absorption, cyst formation, or calcification — depends on the volume of necrosis, its location, and individual tissue response.
The Science of Fat Graft Survival
Why Doesn't All Grafted Fat Survive?
Survival of grafted fat depends on one critical factor: the speed of new blood vessel formation. After fat cells are transplanted to a new location, they must establish new blood supply (neovascularization) with surrounding tissue within 48-72 hours, or they will die from oxygen deprivation.
Factors Affecting Survival Rate:
| Factor | Favorable for Survival | Unfavorable for Survival |
|---|---|---|
| Injection technique | Small volumes, multiple points, fan distribution | Large bolus, concentrated injection |
| Fat processing | Gentle centrifugation, maintained viability | Excessive processing, prolonged exposure |
| Recipient site vascularity | Well-vascularized tissue bed | Scarred tissue, irradiated areas |
| Injection plane | Multi-layer injection | Single-plane large volume |
| Patient factors | Non-smoker, good nutrition | Smoking, diabetes, vascular disease |
| Volume | Appropriate (matched to recipient capacity) | Excessive (beyond recipient nourishment capacity) |
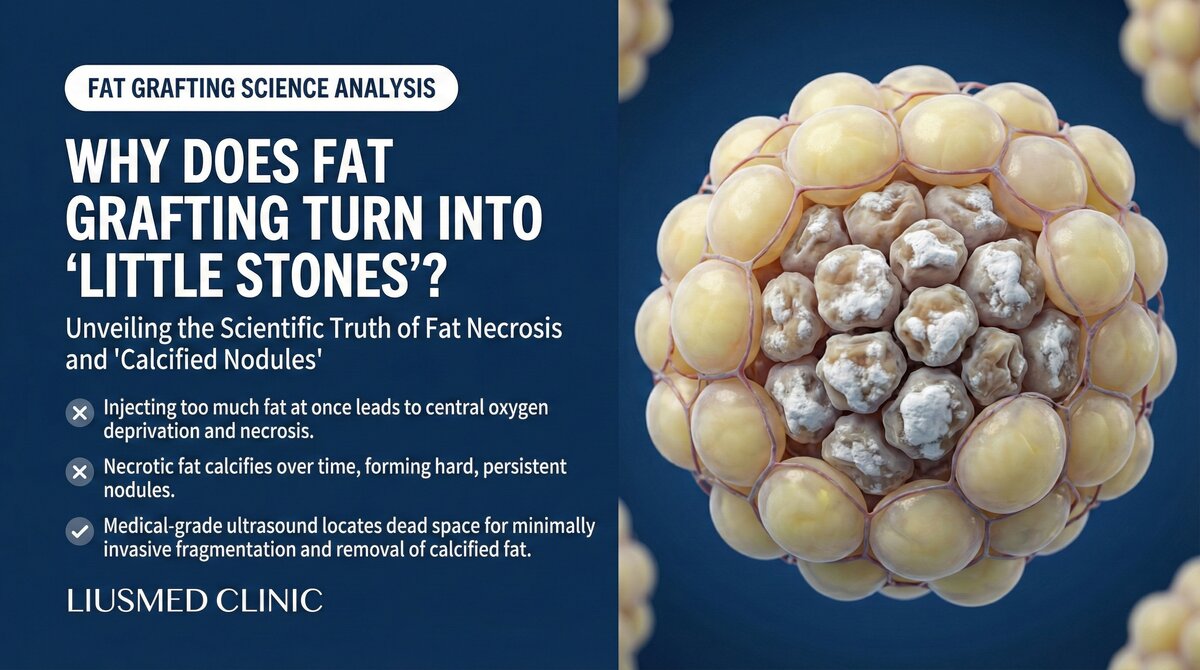
The Three-Zone Theory (Coleman Theory)
A grafted fat bolus can be divided into three concentric zones:
Surviving Zone: The outermost layer, closest to surrounding blood vessels. Fat cells obtain oxygen and nutrients through diffusion before new vessels form, achieving the highest survival rate.
Regenerating Zone: The middle layer. Some fat cells die, but adipose-derived stem cells (ADSCs) may survive and participate in tissue regeneration.
Necrotic Zone: The center of the bolus. Too far from blood vessels to receive any oxygen supply. All fat cells die within days of transplantation.
Key Insight: This is why large-bolus injection carries far higher calcification risk than small-volume multi-point technique — the larger the bolus, the larger the central necrotic zone, and the higher the probability of complications. Understanding this principle is key to prevention.
From Necrosis (irreversible cell/tissue death) to Calcification: The Pathological Progression
Phase 1: Fat Necrosis (Days to Weeks)
Fat cells that fail to survive rupture, releasing intracellular lipids (primarily triglycerides). These free lipids accumulate as oil droplets, stimulating surrounding macrophages to initiate a clearance response.
Phase 2: Oil Cyst Formation (Weeks to Months)
When the volume of necrotic fat exceeds macrophage clearance capacity, free lipids become encapsulated by fibrous tissue, forming oil cysts. The cyst contents are liquid oil, and they feel soft or fluctuant on palpation.
Phase 3: Fibrosis (excess scar tissue formation) and Saponification (Months to Years)
The oil cyst wall gradually undergoes fibrous thickening. In some cases, fatty acids combine with calcium ions in tissue fluid, undergoing saponification — a precursor step to calcification.
Phase 4: Dystrophic Calcification (Months to Years)
Calcium salts deposit in the necrotic tissue, forming dystrophic calcification. This is not caused by systemic calcium metabolism abnormalities but is a local response in necrotic tissue. Calcification patterns include:
- Eggshell calcification: Calcium deposits on the cyst wall, forming a hard shell
- Coarse calcification: Irregular calcified masses
- Microcalcification: Fine, scattered calcification points
Clinical Presentation and Concerns
Palpable Changes
The most common complaint is feeling a hard lump. Unlike lumps from other fillers, fat calcification feels much harder — closer to bone — because it is essentially calcium salt deposition.
Imaging Characteristics
- Ultrasound: Hyperechoic with posterior acoustic shadowing, similar to calcium-based filler appearance on ultrasound
- X-ray/CT: Calcification is directly visible, more intuitive than ultrasound
- MRI (Magnetic Resonance Imaging): Calcification appears as low signal on all sequences; MRI and ultrasound each have advantages
Breast Screening Cross-Interference
Calcification after fat grafting to the breast is a particularly sensitive issue. Fat calcification on mammography can mimic microcalcifications associated with breast cancer, potentially leading to unnecessary biopsies or surgery.
Treatment Challenges of Fat Calcification
Why Is Calcification Especially Difficult to Treat?
Unlike hyaluronic acid, which can be dissolved with hyaluronidase, calcification has no pharmaceutical solution. Treatment options are limited:
Conservative Observation: If calcification is small and asymptomatic, observation is reasonable. However, calcification typically does not resolve spontaneously.
Surgical Excision: Larger calcified masses may require surgical removal. But facial surgery carries scarring risks, and widely distributed calcification is difficult to completely remove.
Ultrasound-Guided Precision Treatment: Under high-resolution ultrasound guidance, calcification can be precisely located and treated through minimally invasive approaches. This is currently the most accurate method, but requires the operator to have experience in ultrasound-guided intervention. Learn more about filler extraction techniques.
| Treatment | Indicated For | Advantages | Limitations |
|---|---|---|---|
| Conservative observation | Small, asymptomatic | Non-invasive | No improvement |
| Surgical excision | Large, localized | Complete removal possible | Scarring risk |
| Ultrasound-guided minimally invasive | Most situations | Precise, minimally invasive | Requires specialized equipment and skill |
Prevention Strategies
The core of preventing fat calcification is improving fat survival and reducing necrosis:
- Small-volume, multi-point injection technique: Small amounts at each injection point to increase vascular contact surface area
- Multi-layer injection: Avoid forming large boluses in a single plane
- Appropriate volume: Avoid overfilling; consider the recipient site's vascular nourishment capacity
- Gentle fat processing: Minimize ex-vivo damage to fat
- Post-operative care: Avoid compressing the grafted area; maintain good blood circulation
Learn more about pillow face correction and the filler repair evaluation process. If you are experiencing hard lumps after fat grafting, contact us for an assessment.
Key Insight: Managing autologous fat grafting complications is often more challenging than synthetic filler complications — there is no dissolving enzyme available, and once calcification forms, it cannot be treated with medication. This does not mean fat grafting is bad, but reminds us: any filling method has its own unique risk profile, and the precision of technique directly influences complication rates.
Common questions
Does fat grafting to the face always calcify?
No. Calcification is tied to whether the fat survives. Roughly 30 to 70 percent of grafted fat takes, and the part that doesn't is what the body has to clear. Most of it gets reabsorbed, and only some of it goes on to form an oil cyst or calcify. Using small volumes at multiple points and layering the injection keeps more fat alive, which brings that risk down.
Does a calcified lump feel the same as a lump from other fillers?
Usually it feels harder. Fat calcification is essentially calcium salt deposition, so it sits closer to bone in firmness, which is different from the softer lump you might get with hyaluronic acid. To actually confirm it, ultrasound, X-ray or CT shows the calcification more reliably than feeling for it by hand.
Can a dissolving injection or medication break down fat calcification?
It can't. Hyaluronic acid has hyaluronidase to dissolve it, but there is no medication that dissolves calcification. What we do depends on the situation: small, symptom-free ones can be watched, larger ones may need surgical removal, or it can be treated precisely through a minimally invasive approach under high-resolution ultrasound guidance.
Will the calcification go away on its own?
Generally no. Once calcification forms it usually doesn't resolve by itself. If it's small and not causing symptoms, we can observe and follow it, but it tends not to improve on its own — which is why the emphasis is on protecting fat survival at the time of injection so less necrotic fat is left behind.
How can I lower the chance of calcification after fat grafting?
The key is keeping as much fat alive as possible and leaving less dead tissue behind. That means small amounts at each point, injecting in multiple layers, not overfilling beyond what the area can nourish, handling the fat gently, and after surgery avoiding pressure on the grafted area while keeping good circulation. The finer the technique, the lower the chance of problems.
Related Services

Specialties
Credentials
- Kaohsiung Medical University, School of Medicine
- Attending Physician, Dermatology, Kaohsiung Chang Gung Memorial Hospital
- Attending Physician, Aesthetic Center, Kaohsiung Chang Gung Memorial Hospital
- Visiting Physician, Dermatology, Xiamen Chang Gung Hospital
- Visiting Physician, Aesthetic Center, Xiamen Chang Gung Hospital
"For every surgery, I strive to achieve a good outcome through a small incision and refined technique. Minimally invasive surgery is not just a technique — it's a commitment of respect to every patient."
Recovery after any procedure needs peer support too
Want to learn more?
Schedule a consultation for professional evaluation and advice